SOME PHYSICIAN WORK FOR FREE
By Staff Reporters
SPONSOR: http://www.MarcinkoAssociates.com
***

***
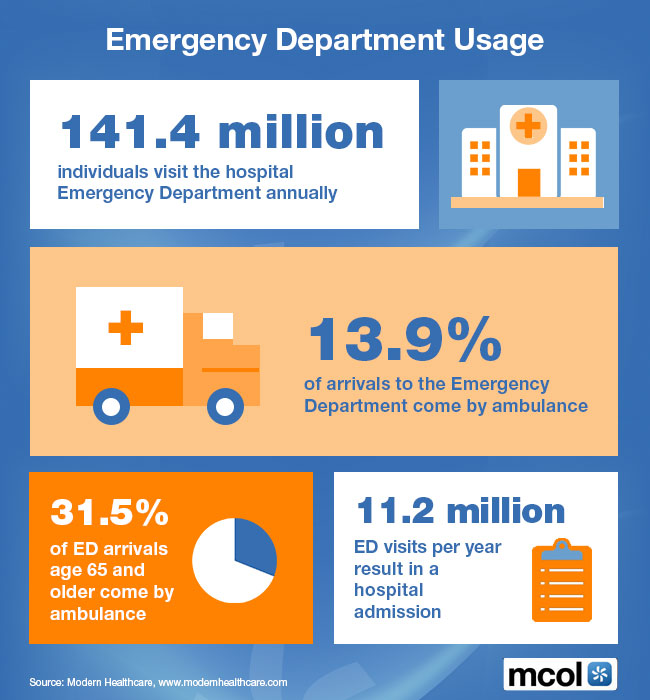
What is an Emergency Medicine Physician?
An emergency medicine physician is a medical doctor who specializes in the diagnosis, treatment, and management of acute and life-threatening medical conditions that require immediate intervention. These physicians work in hospital emergency departments, urgent care centers, and other acute care settings, where they provide rapid assessment, stabilization, and treatment to patients of all ages with a wide range of medical emergencies.
Emergency medicine physicians are trained to handle diverse medical emergencies, including trauma, cardiac emergencies, respiratory distress, severe infections, neurological emergencies, and obstetric emergencies, among others. They play a vital role in the front line management of medical emergencies, ensuring that patients receive prompt and appropriate care to improve outcomes and save lives.
***
Classic: Emergent Room or Emergency Department care is the provision of immediate medical service offering outpatient care for the treatment of acute and chronic illness and injury. It requires a broad and comprehensive fund of knowledge to provide such care. Excellence in care for patients with complex and or unusual conditions is founded on the close communication and collaboration between the urgent care medicine physician, the specialists and the primary physicians.
Modern: Urgent care does not replace your primary care physician. An urgent care center is a convenient option when someone’s regular physician is on vacation or unable to offer a timely appointment. Or, when illness strikes outside of regular office hours, urgent care offers an alternative to waiting for hours in a hospital Emergency Room.
Examples: Chest pain, bleeding that cannot be stopped and loss of consciousness; etc.
***
***
SOME ER DOCTORS WORK FOR FREE
The new president of emergency medicine for the Alberta Medical Association says Emergency Room physicians already coping with long hours, staff shortages and jammed waiting rooms are also being obligated, in some cases, to work for free. Dr. Warren Thirsk says the government has yet to follow through on a promise to reimburse emergency room doctors for so-called “good faith” payments.
“There’s been lots of excuses, but the bottom line is no one has actually received a penny for those suspended good-faith payments,” Thirsk said in an interview. “On average, every emergency physician in this province is out thousands of dollars for free work.” Good-faith payments reimburse ER doctors when they see patients who don’t have identification and can’t prove an Alberta Health Care Insurance Plan billing number.
Thirsk said the United Conservative government stopped those payments when it ripped up the master agreement with the AMA in early 2020. He said it promised to bring back those payments when the two sides agreed to a new deal in September 2022. But to date that hasn’t happened, he said.
“I’m legally and morally bound to look after you [if] you’re unidentified [as a patient],” said Thirsk, an emergency room doctor at Edmonton’s Royal Alexandra Hospital.
“I’m going to look after you because it’s the right thing to do no matter what the problem is.”
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Like and Refer
***
***
Share this:

Filed under: "Doctors Only", Ask a Doctor, Drugs and Pharma, Ethics, Health Economics, Health Insurance, LifeStyle, Managed Care, Marcinko Associates | Tagged: Alberta Medical Association, DO, doctor salary, ED, emergency department, emergency medicine, emergency room, ER, er doctor pay, ER physicians, health, Health Economics, Health Insurance, healthcare, Healthcare Finance, insurance, Marcinko, MD, mental health, physician, pro bono medical care, trauma, warren thirsk | Leave a comment »