HEALTHCARE DEFINITIONS
By Staff Reporters
SPONSOR: http://www.CertifiedMedicalPlanner.org
***

***
When you visit health clinic or hospital for a medical appointment, you’ll be seen by a doctor, healthcare provider and/or medical prescriber. But what do these words really mean?
***
***
Doctors / Physicians
Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Doctor of Osteopathy (DO, or Doctor of Dental Surgery (DDS/DMD). Doctors, also known as physicians, have extensive prescription privileges across various specialties. They can diagnose medical conditions, prescribe medication, and oversee the overall management of patient care. Doctors include general practitioners, specialists such as cardiologists or dermatologists, and surgeons. Their prescription authority encompasses a wide range of medications to address acute and chronic health conditions, ranging from antibiotics to specialized treatments for complex diseases.
MORE: https://medicalexecutivepost.com/2023/06/17/the-md-versus-do-degree/
***
***
Medical Providers
A medical provider is a general term that encompasses a wide range of education levels, skill-sets, and specializations. A provider could be a Physician Assistant (PA), Nurse Practitioner (NP), Clinical Nurse Specialist (CNS), Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Dentist (DDSDMD) or Doctor of Osteopathy (DO).
***
Medical Drug Prescribers
Generally, psychologists and therapists do not have prescription privileges. They focus on psychotherapy and counseling rather than medication management. However, some jurisdictions may grant limited prescription rights to psychologists who undergo additional training and certification. Like psychologists, therapists typically do not have prescription privileges. They focus on providing counseling and psychotherapy to address mental health issues and emotional concerns.
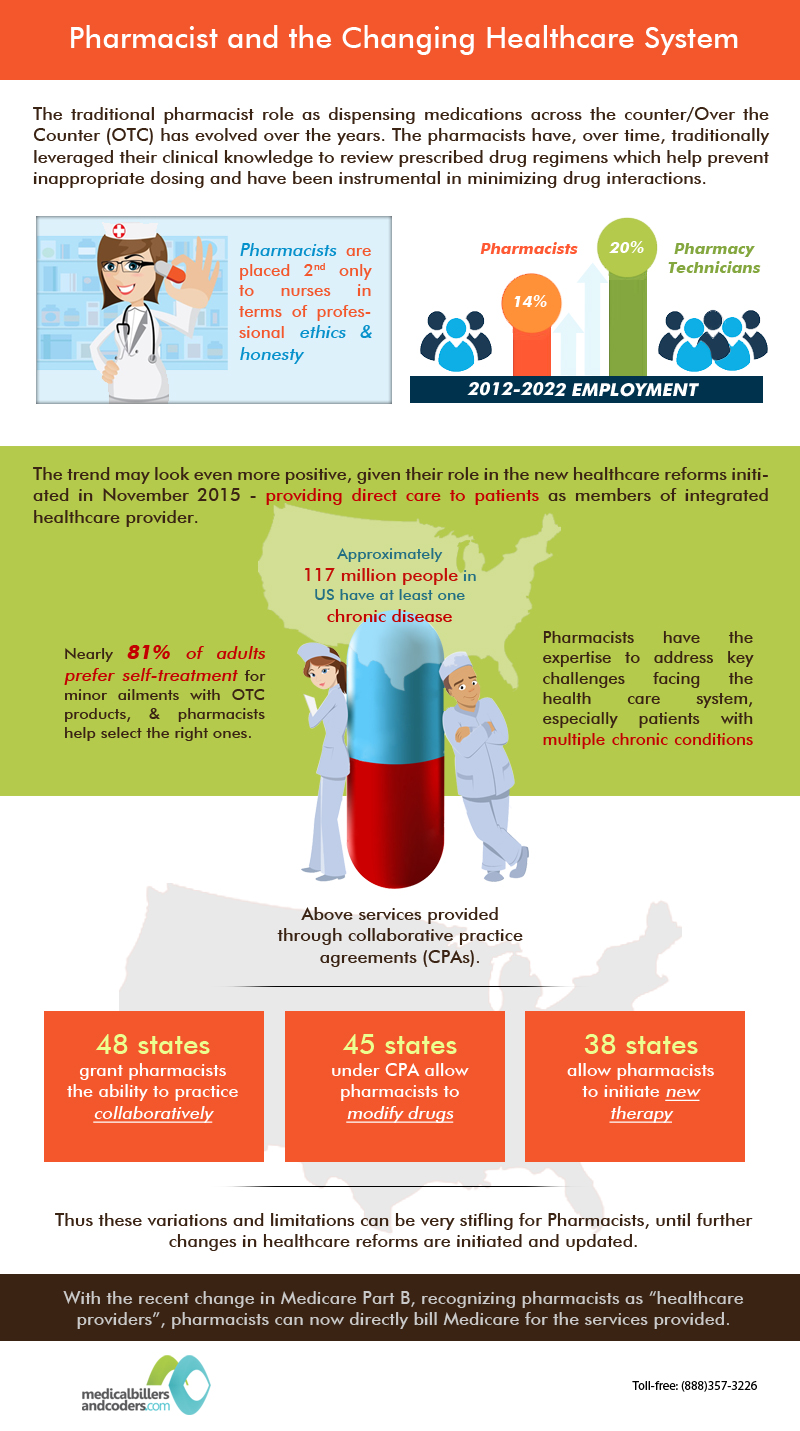
PHARMACISTS: https://medicalexecutivepost.com/2025/02/12/pharmd-doctor-of-pharmacy/
Psychiatrists are medical doctors (MD/DO) who specialize in the diagnosis and treatment of mental health disorders. They have full prescription privileges and can prescribe a wide range of medications to manage psychiatric conditions.
In most cases, physical therapists do not have the authority to prescribe medication. They primarily focus on rehabilitation and physical interventions to improve mobility and function.
MORE: https://medicalexecutivepost.com/2025/02/23/doctorate-physical-therapy/
Nurse practitioners are advanced practice nurses with the authority to diagnose, treat, and prescribe medication independently in many states and countries. They undergo extensive education and training, which allows them to provide a wide range of healthcare services, including medication management.
Similar to nurse practitioners, psychiatric nurse practitioners have the authority to prescribe medication for mental health conditions. They specialize in psychiatric and mental health care, offering comprehensive treatment that may include medication management.
Chiropractors primarily focus on diagnosing and treating musculoskeletal disorders through manual adjustments and therapies. They do not have surgical or prescription privileges in most jurisdictions.
Optometrists are trained to diagnose and treat vision problems, including prescribing corrective lenses and medications for certain eye conditions such as infections or inflammation.
Registered nurses typically do not have prescription privileges. They work under the direction of physicians and nurse practitioners, assisting with patient care but not prescribing medication themselves.
Dentists have limited prescription privileges related to dental care, such as antibiotics or pain medications for dental procedures. However, they do not have the authority to prescribe general medications outside of their scope of practice.
Nutritionists typically do not have prescription privileges. They specialize in providing dietary advice and counseling to promote health and well-being through nutrition but do not prescribe medication.
Depending on their scope of practice and legal regulations in their jurisdiction, nurse midwives may have limited prescription privileges for certain medications related to prenatal care, childbirth, and postpartum care.
MORE: http://www.HealthDictionarySeries.org
COMMENTS APPRECIATED
Like and Refer
***
***
Share this:

Filed under: Ask a Doctor, Career Development, Drugs and Pharma, Health Economics, Health Law & Policy, Healthcare Finance | Tagged: DC, DDS, dentist, dictionary, DMD, DO, Drugs, health, health dictionary, healthcare, LPN, MD, medicine, midwife, news, NP, nurse, nursing, nutritionists, OD, osteopthy, PA, PBMs, pharmacists, pmb, podiatry, providers, RN, Rx, surgery, Technology, therapist | Leave a comment »