Radiation Safety Concerns
By Michael Grabell
ProPublica, November 1st, 2011, 1:06 pm
On Sept. 23rd, 1998, a panel of radiation safety experts gathered at a Hilton hotel in Maryland to evaluate a new device that could detect hidden weapons and contraband. The machine, known as the Secure 1000, beamed X-rays at people to see underneath their clothing.
One after another, the experts convened by the Food and Drug Administration raised questions about the machine because it violated a longstanding principle in radiation safety — that humans shouldn’t be X-rayed unless there is a medical benefit.
“I think this is really a slippery slope,” said Jill Lipoti, who was the director of New Jersey’s radiation protection program. The device was already deployed in prisons; what was next, she and others asked — courthouses, schools, airports? “I am concerned … with expanding this type of product for the traveling public,” said another panelist, Stanley Savic, the vice president for safety at a large electronics company. “I think that would take this thing to an entirely different level of public health risk.”
The machine’s inventor, Steven W. Smith, assured the panelists that it was highly unlikely that the device would see widespread use in the near future. At the time, only 20 machines were in operation in the entire country.
“The places I think you are not going to see these in the next five years is lower-security facilities, particularly power plants, embassies, courthouses, airports and governments,” Smith said. “I would be extremely surprised in the next five to 10 years if the Secure 1000 is sold to any of these.”
US Marching Millions thru Body Scanners
Today, the United States has begun marching millions of airline passengers through the X-ray body scanners, parting ways with countries in Europe and elsewhere that have concluded that such widespread use of even low-level radiation poses an unacceptable health risk. The government is rolling out the X-ray scanners despite having a safer alternative that the Transportation Security Administration says is also highly effective.
ProPublica Investigates
A ProPublica/PBS NewsHour investigation of how this decision was made shows that in post-9/11America, security issues can trump even long-established medical conventions. The final call to deploy the X-ray machines was made not by the FDA, which regulates drugs and medical devices, but by the TSA, an agency whose primary mission is to prevent terrorist attacks.
Research suggests that anywhere from six to 100 U.S.airline passengers each year could get cancer from the machines. Still, the TSA has repeatedly defined the scanners as “safe,” glossing over the accepted scientific view that even low doses of ionizing radiation — the kind beamed directly at the body by the X-ray scanners — increase the risk of cancer.
“Even though it’s a very small risk, when you expose that number of people, there’s a potential for some of them to get cancer,” said Kathleen Kaufman, the former radiation management director in Los AngelesCounty, who brought the prison X-rays to the FDA panel’s attention.
About 250 X-ray scanners are currently in U.S.airports, along with 264 body scanners that use a different technology, a form of low-energy radio waves known as millimeter waves.
Robin Kane, the TSA’s assistant administrator for security technology, said that no one would get cancer because the amount of radiation the X-ray scanners emit is minute. Having both technologies is important to create competition, he added.
“It’s a really, really small amount relative to the security benefit you’re going to get,” Kane said. “Keeping multiple technologies in play is very worthwhile for the U.S.in getting that cost-effective solution — and being able to increase the capabilities of technology because you keep everyone trying to get the better mousetrap.”
Determined to fill a critical hole in its ability to detect explosives, the TSA plans to have one or the other operating at nearly every security lane in America by 2014. The TSA has designated the scanners for “primary” screening: Officers will direct every passenger, including children, to go through either a metal detector or a body scanner, and the passenger’s only alternative will be to request a physical pat-down.
How did the United States swing from considering such X-rays taboo to deeming them safe enough to scan millions of people a year?
A new wave of terrorist attacks using explosives concealed on the body, coupled with the scanners’ low dose of radiation, certainly convinced many radiation experts that the risk was justified.
But other factors helped the machines gain acceptance.
Gaining Acceptance
Because of a regulatory Catch-22, the airport X-ray scanners have escaped the oversight required for X-ray machines used in doctors’ offices and hospitals. The reason is that the scanners do not have a medical purpose, so the FDA cannot subject them to the rigorous evaluation it applies to medical devices.
Still, the FDA has limited authority to oversee some non-medical products and can set mandatory safety regulations. But the agency let the scanners fall under voluntary standards set by a nonprofit group heavily influenced by industry.
As for the TSA, it skipped a public comment period required before deploying the scanners. Then, in defending them, it relied on a small body of unpublished research to insist the machines were safe, and ignored contrary opinions from U.S. and European authorities that recommended precautions, especially for pregnant women. Finally, the manufacturer, Rapiscan Systems, unleashed an intense and sophisticated lobbying campaign, ultimately winning large contracts.
Both the FDA and TSA say due diligence has been done to assure the scanners’ safety. Rapiscan says it won the contract because its technology is superior at detecting threats. While the TSA says X-ray and millimeter-wave scanners are both effective, Germanydecided earlier this year not to roll out millimeter-wave machines after finding they produced too many false positives.
Most of the news coverage on body scanners has focused on privacy, because the machines can produce images showing breasts and buttocks. But the TSA has since installed software to make the images less graphic. While some accounts have raised the specter of radiation, this is the first report to trace the history of the scanners and document the gaps in regulation that allowed them to avoid rigorous safety evaluation.
Little research on Cancer Risk
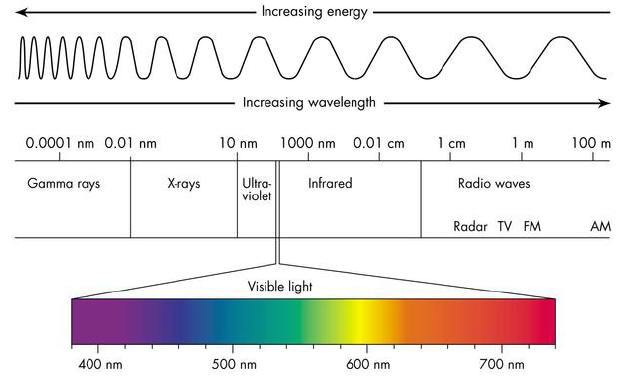
Humans are constantly exposed to ionizing radiation, a form of energy that has been shown to strip electrons from atoms, damage DNA and mutate genes, potentially leading to cancer. Most radiation comes from radon, a gas produced from naturally decaying elements in the ground. Another major source is cosmic radiation from outer space. Many common items, such as smoke detectors, contain tiny amounts of radioactive material, as do exit signs in schools and office buildings.
As a result, the cancer risk from any one source of radiation is often small. Outside of nuclear accidents, such as that at Japan’s Fukushima plant, and medical errors, the health risk comes from cumulative exposure.
In Rapiscan’s Secure 1000 scanner, which uses ionizing radiation, a passenger stands between two large blue boxes and is scanned with a pencil X-ray beam that rapidly moves left to right and up and down the body. In the other machine, ProVision, made by defense contractor L-3 Communications, a passenger enters a chamber that looks like a round phone booth and is scanned with millimeter waves, a form of low-energy radio waves, which have not been shown to strip electrons from atoms or cause cancer.
Only a decade ago, many states prohibited X-raying a person for anything other than a medical exam. Even after 9/11, such non-medical X-raying remains taboo in most of the industrialized world. In July, the European Parliament passed a resolution that security “scanners using ionizing radiation should be prohibited” because of health risks. Although the United Kingdom uses the X-ray machine for limited purposes, such as when passengers trigger the metal detector, most developed countries have decided to forgo body scanners altogether or use only the millimeter-wave machines.
While the research on medical X-rays could fill many bookcases, the studies that have been done on the airport X-ray scanners, known as backscatters, fill a file no more than a few inches thick. None of the main studies cited by the TSA has been published in a peer-reviewed journal, the gold standard for scientific research.
Those tests show that the Secure 1000 delivers an extremely low dose of radiation, less than 10 microrems. The dose is roughly one-thousandth of a chest X-ray and equivalent to the cosmic radiation received in a few minutes of flying at typical cruising altitude. The TSA has used those measurements to say the machines are “safe.”
Most of what researchers know about the long-term health effects of low levels of radiation comes from studies of atomic bomb survivors in Hiroshima and Nagasaki. By charting exposure levels and cancer cases, researchers established a linear link that shows the higher the exposure, the greater risk of cancer.
Some scientists argue the danger is exaggerated. They claim low levels stimulate the repair mechanism in cells, meaning that a little radiation might actually be good for the body.
National Academy of Sciences
But, in the authoritative report on low doses of ionizing radiation, published in 2006, the National Academy of Sciences reviewed the research and concluded that the preponderance of research supported the linear link. It found “no compelling evidence” that there is any level of radiation at which the risk of cancer is zero.
Radiation experts say the dose from the backscatter is negligible when compared to naturally occurring background radiation. Speaking to the 1998 FDA panel, Smith, the inventor, compared the increased risk to choosing to visit Denver instead of San Diegoor the decision to wear a sweater versus a sport coat.
Using the linear model, even such trivial amounts increase the number of cancer cases. Rebecca Smith-Bindman, a radiologist at the University of California, San Francisco, estimated that the backscatters would lead to only six cancers over the course of a lifetime among the approximately 100 million people who fly every year. David Brenner, director of Columbia University’s Center for Radiological Research, reached a higher number — potentially 100 additional cancers every year.
“Why would we want to put ourselves in this uncertain situation where potentially we’re going to have some cancer cases?” Brenner asked. “It makes me think, really, why don’t we use millimeter waves when we don’t have so much uncertainty?”
But even without the machines, Smith-Bindman said, the same 100 million people would develop 40 million cancers over the course of their lifetimes. In this sea of cancer cases, it would be impossible to identify the patients whose cancer is linked to the backscatter machines.
How the scanners avoided strict oversight
Although they deliberately expose humans to radiation, the airport X-ray scanners are not medical devices, so they are not subject to the stringent regulations required for diagnostic X-ray machines.
If they were, the manufacturer would have to submit clinical data showing safety and effectiveness and be approved through a rigorous process by the FDA. If the machines contained radioactive material, they would have to report to the Nuclear Regulatory Commission.
But because it didn’t fit into either category, the Secure 1000 was classified as an electronic product. The FDA does not review or approve the safety of such products. However, manufacturers must provide a brief radiation safety report explaining the dose and notify the agency if any overexposure is discovered. According to the FDA, no such incidents have been reported.
Under its limited oversight of electronic products, the FDA could issue mandatory safety regulations. But it didn’t do so, a decision that flows from its history of supervising electronics.
Regulation of electronic products in the United States began after a series of scandals. From the 1930s to the 1950s, it was common for a child to go to a shoe store and stand underneath an X-ray machine known as a fluoroscope to check whether a shoe was the right fit. But after cases arose of a shoe model’s leg being amputated and store clerks developing dermatitis from putting their hands in the beam to adjust the shoe, the practice ended.
In 1967, General Electric recalled 90,000 color televisions that had been sold without the proper shielding, potentially exposing viewers to dangerous levels of radiation. The scandal prompted the creation of the federal Bureau of Radiological Health.
“That ultimately led to a lot more aggressive program,” said John Villforth, who was the director of the bureau. Over the next decade, the bureau created federal safety standards for televisions, medical X-rays, microwaves, tanning beds, even laser light shows.
But in 1982, the FDA merged the radiological health bureau into its medical-device unit.
“I was concerned that if they were to combine the two centers into one, it would probably mean the ending of the radiation program because the demands for medical-device regulation were becoming increasingly great,” said Villforth, who was put in charge of the new Center for Devices and Radiological Health. “As I sort of guessed, the radiation program took a big hit.”
The new unit became stretched for scarce resources as it tried to deal with everything from tongue depressors to industrial lasers. The government used to have 500 people examining the safety of electronic products emitting radiation. It now has about 20 people. In fact, the FDA has not set a mandatory safety standard for an electronic product since 1985.
As a result, there is an FDA safety regulation for X-rays scanning baggage — but none for X-rays scanning people at airports.
Meanwhile, scientists began developing backscatter X-rays, in which the waves are reflected off an object to a detector, for the security industry.
The Secure 1000 people scanner was invented by Smith in 1991 and later sold to Rapiscan, then a small security firm based in southern California. The first major customer was the California prison system, which began scanning visitors to prevent drugs and weapons from getting in. But the state pulled the devices in 2001 after a group of inmates’ wives filed a class-action lawsuit accusing the prisons of violating their civil liberties.
***

***
US Customs Service
The U.S. Customs Service deployed backscatter machines for several years but in limited fashion and with strict supervision. Travelers suspected of carrying contraband had to sign a consent form, and Customs policy prohibited the scanning of pregnant women. The agency abandoned them in 2006, not for safety reasons but because smugglers had learned where the machines were installed and adapted their methods to avoid them, said Rick Whitman, the radiation safety officer for Customs until 2008.
Yet, even this limited application of X-ray scanning for security dismayed radiation safety experts. In 1999, the Conference of Radiation Control Program Directors, a nongovernmental organization, passed a resolution recommending that such screening be stopped immediately.
The backscatter machines had also caught the attention of the 1998 FDA advisory panel, which recommended that the FDA establish government safety regulations for people scanners. Instead, the FDA decided to go with a voluntary standard set by a trade group largely comprising manufacturers and government agencies that wanted to use the machines.
“Establishing a mandatory standard takes an enormous amount of resources and could take a decade to publish,” said Dan Kassiday, a longtime radiation safety engineer at the FDA.
In addition, since the mid-1990s, Congress has directed federal safety agencies to use industry standards wherever possible instead of creating their own.
The FDA delegated the task of establishing the voluntary standards to the American National Standards Institute. A private nonprofit that sets standards for many industries, ANSI convened a committee of the Health Physics Society, a trade group of radiation safety specialists. It was made up of 15 people, including six representatives of manufacturers of X-ray body scanners and five from U.S. Customs and the California prison system. There were few government regulators and no independent scientists.
In contrast, the FDA advisory panel was also made up of 15 people — five representatives from government regulatory agencies, four outside medical experts, one labor representative and five experts from the electronic products industry, but none from the scanner manufacturers themselves.
“I am more comfortable with having a regulatory agency — either federal or the states — develop the standards and enforce them,” Kaufman said. Such regulators, she added, “have only one priority, and that’s public health.”
A representative of the Health Physics Society committee said that was its main priority as well. Most of the committee’s evaluation was completed before 9/11. The standard was published in 2002 and updated with minor changes in 2009.
Ed Bailey, chief of California’s radiological health branch at the time, said he was the lone voice opposing the use of the machines. But after 9/11, his views changed about what was acceptable in pursuit of security.
“The whole climate of their use has changed,” Bailey said. “The consequence of something being smuggled on an airplane is far more serious than somebody getting drugs into a prison.”
Are Inspections Independent?
While the TSA doesn’t regulate the machines, it must seek public input before making major changes to security procedures. In July, a federal appeals court ruled that the agency failed to follow rule-making procedures and solicit public comment before installing body scanners at airports across the country. TSA spokesman Michael McCarthy said the agency couldn’t comment on ongoing litigation.
The TSA asserts there is no need to take additional precautions for sensitive populations, even pregnant women, following the guidance of the congressionally chartered National Council on Radiation Protection & Measurements.
But other authorities have come to the opposite conclusion. A report by France’s radiation safety agency specifically warned against screening pregnant women with the X-ray devices. In addition, the Federal Aviation Administration’s medical institute has advised pregnant pilots and flight attendants that the machine, coupled with their time in the air, could put them over their occupational limit for radiation exposure and that they might want to adjust their work schedules accordingly.
No similar warning has been issued for pregnant frequent fliers.
Even as people scanners became more widespread, government oversight actually weakened in some cases.
Inspections of X-ray equipment in hospitals and industry are the responsibility of state regulators — and before 9/11, many states also had the authority to randomly inspect machines in airports. But that ended when the TSA took over security checkpoints from the airlines.
Instead, annual inspections are done by Rapiscan, the scanners’ manufacturer.
“As a regulator, I think there’s a conflict of interest in having the manufacturer and the facility inspect themselves,” Kaufman said.
Last year, in reaction to public anger from members of Congress, passengers and advocates, the TSA contracted with the Army Public Health Command to do independent radiation surveys. But email messages obtained in a lawsuit brought by the Electronic Privacy Information Center, a civil liberties group, raise questions about the independence of the Army surveys.
One email sent by TSA health and safety director Jill Segraves shows that local TSA officials were given advance notice and allowed to “pick and choose” which systems the Army could check.
That email also suggests that Segraves considered the Army inspectors a valuable public-relations asset: “They are our radiation myth busters,” she wrote to a local security director.
Some TSA screeners are concerned about their own radiation exposure from the backscatters, but the TSA has not allowed them to wear badges that could measure it, said Milly Rodriguez, health and safety specialist for the American Federation of Government Employees, which represents TSA officers.
“We have heard from members that sometimes the technicians tell them that the machines are emitting more radiation than is allowed,” she said.
McCarthy, the TSA spokesman, said the machines are physically incapable of producing radiation above the industry standard. In the email, he said, the inspections allow screeners to ask questions about radiation and address concerns about specific machines.
TSA Video: http://en.wikipedia.org/wiki/File:TSA-_How_It_Works.ogv
The company’s lobbying campaign
While the TSA maintains that the body scanners are essential to preventing attacks on airplanes, it only began rolling them out nine years after 9/11.
After the attempted shoe-bombing in December 2001, the federal government conducted a trial of a Rapiscan backscatter at the Orlando International Airport. But the revealing images drew protests that the machines amounted to a virtual strip search.
The TSA considered the scanners again after two Chechen women blew up Russian airliners in 2004. Facing a continued outcry over privacy, the TSA instead moved forward with a machine known as a “puffer” because it released several bursts of air on the passengers’ clothes and analyzed the dislodged particles for explosives. But after discovering the machines were ineffective in the field and difficult to maintain, the TSA canceled the program in 2006.
Around that time, Rapiscan began to beef up its lobbying on Capitol Hill. It opened a Washington,D.C., office and, according to required disclosures, more than tripled its lobbying expenditures in two years, from less than $130,000 in 2006 to nearly $420,000 in 2008. It hired former legislative aides to Rep. David Price, D-N.C., then chairman of the homeland security appropriations subcommittee, and to Sen. Trent Lott, R-Miss.
It started a political action committee and began contributing heavily to Price; Rep. Bennie Thompson, D-Miss., then head of the homeland security committee; Rep. Jane Harman, D-Calif., also on that committee; and Sen. Thad Cochran, R-Miss., the top Republican on the Senate appropriations committee.
In addition, it opened a new North Carolina plant in Price’s district and expanded its operations in Ocean Springs, Miss., and at its headquarters in Torrance, Calif., in Harman’s district.
“Less than a month after U.S. Senator Trent Lott and other local leaders helped officially open Rapiscan Systems’ new Ocean Springs factory,” Lott’s office announced in a news release in late 2006, “the company has won a $9.1 million Department of Defense contract.”
But Rapiscan still hadn’t landed a major contract to roll out its X-ray body scanners in commercial airports. Indeed, in 2007, with new privacy filters in place, the TSA began a trial of millimeter-wave and backscatter machines at several major airports, after which the agency opted to go with the millimeter-wave machines. The agency said health concerns weren’t a factor.
But with the 2009 federal stimulus package, which provided $300 million for checkpoint security machines, the TSA began deploying backscatters as well. Rapiscan won a $173 million, multiyear contract for the backscatters, with an initial $25 million order for 150 systems to be made inMississippi.
Three other companies — American Science & Engineering, Tek84 Engineering Group and Valley Forge Composite Technologies — make X-ray scanners, but none are used by the TSA. Peter Kant, executive vice president for Rapiscan, said the company expanded its lobbying because its business was increasingly affected by the government.
“There’s a lot of misinformation about the technology; there’s a lot of questions about how various inspection technologies work,” he said. “And we needed a way to be able to provide that information and explain the technology and how it works, and that’s what lobbying is.”
The lawmakers either declined to comment or said the lobbying, campaign contributions and local connections had nothing to do with the TSA’s decision to purchase Rapiscan machines. The TSA said the contract was bid competitively and that the winning machines had to undergo comprehensive research and testing phases before being deployed.
While the scanners were appearing in more and more airports, few passengers went through them, because they were used mostly for random screening or to resolve alarms from the metal detector.
That changed on Christmas Day 2009, when a Nigerian man flying toDetroittried to ignite a pouch of explosives hidden in his underwear.
Following the foiled “Great Balls of Fire” suicide bombing, as the New York Post dubbed it, Homeland Security Secretary Janet Napolitano ramped up plans to roll out body scanners nationwide. Members of Congress and aviation security experts also pushed heavily for the TSA to install more machines that could detect explosives on passengers.
Harman sent a letter to Napolitano, noting that Rapiscan was in her district.
“I urge you to expedite installation of scanning machines in key airports,” Harman wrote in the letter, which was first reported by the website CounterPunch. “If you need additional funds, I am ready to help.”
Michael Chertoff, who had supported body scanners while secretary of Homeland Security, appeared frequently on TV advocating their use. In one interview, he disclosed that his consulting firm, Chertoff Group, had done work for Rapiscan, sparking accusations that he was trying to profit from his time as a government servant.
Despite the criticism, little has been revealed about the relationship. Rapiscan dismissed it, asserting that the consulting work had to do with international cargo and port security issues — not aviation.
“There was nothing that was not above board,” Kant said. “His comments about passenger screening and these machines were simply his own and was nothing that we had engaged the Chertoff Group for.”
In a statement, the Chertoff Group said it “played no role in the sale of whole body imaging technology to TSA” and that Chertoff “was in no way compensated for his public statements.”
A public records request by ProPublica turned up empty: The Department of Homeland Security said it could not find any correspondence to or from Chertoff related to body scanners. DHS also said Chertoff did not use email.
Assessment
The TSA plans to deploy 1,275 backscatter and millimeter-wave scanners covering more than half its security lanes by the end of 2012 and 1,800 covering nearly all the lanes by 2014.
According to annual reports filed with the Securities and Exchange Commission, OSI Systems, the parent company of Rapiscan, has seen revenue from its security division more than double since 2006 to nearly $300 million in fiscal year 2011.
Link: http://www.propublica.org/article/u.s.-government-glossed-over-cancer-concerns-as-it-rolled-out-airport-x-ray.
Miles O’Brien and Kate Tobin of PBS News Hour contributed to this report.
Related Stories:
New Army Study Says Radiation From Airport Body Scanners Is Minor
by Michael Grabell, ProPublica, July 14
TSA Airport Scanners Wouldn’t Catch an Implant Bomber
by Michael Grabell, ProPublica, July 6
Scientists Cast Doubt on TSA Tests of Full-Body Scanners
by Michael Grabell, ProPublica, May 16
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Our Other Print Books and Related Information Sources:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Healthcare Organizations: www.HealthcareFinancials.com
Physician Advisors: www.CertifiedMedicalPlanner.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Sponsors Welcomed: And, credible sponsors and like-minded advertisers are always welcomed.
Link: https://healthcarefinancials.wordpress.com/2007/11/11/advertise






Filed under: Breaking News, Ethics, Quality Initiatives | Tagged: Airport X-Ray Scanners, Body Scanners, Bureau of Radiological Health, Health Physics Society, Jill Lipoti, L-3 Communications, Michael Chertoff, Michael Grabell, millimeter-wave machines, ProVision, Radiation Safety Concerns, Rapiscan Systems, Secure 1000, TSA | 6 Comments »











 A few days ago, Daniel Palestrant MD, Founder of par8o & SERMO, compared the American healthcare system to a patient with cancer.
A few days ago, Daniel Palestrant MD, Founder of par8o & SERMO, compared the American healthcare system to a patient with cancer. Assessment
Assessment































































































{kind=link}
{kind=link}