BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on December 8, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
CVS is overhauling how it prices prescription drugs
In a recent announcement, the company CVS promised that its new model would be more transparent than the current setup, which prices drugs based on complex reimbursement formulas that can make the costs of prescriptions confusing for consumers.
The new model, called CVS CostVantage, is based on a simple equation: Drugs will cost what CVS paid for them, plus a limited markup and a flat fee to cover the services of fulfilling the prescriptions. That’s similar to a plan proposed by billionaire Mark Cuban, founder of Cost Plus Drugs, to bring accountability to drug pricing in the US.
Posted on May 7, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
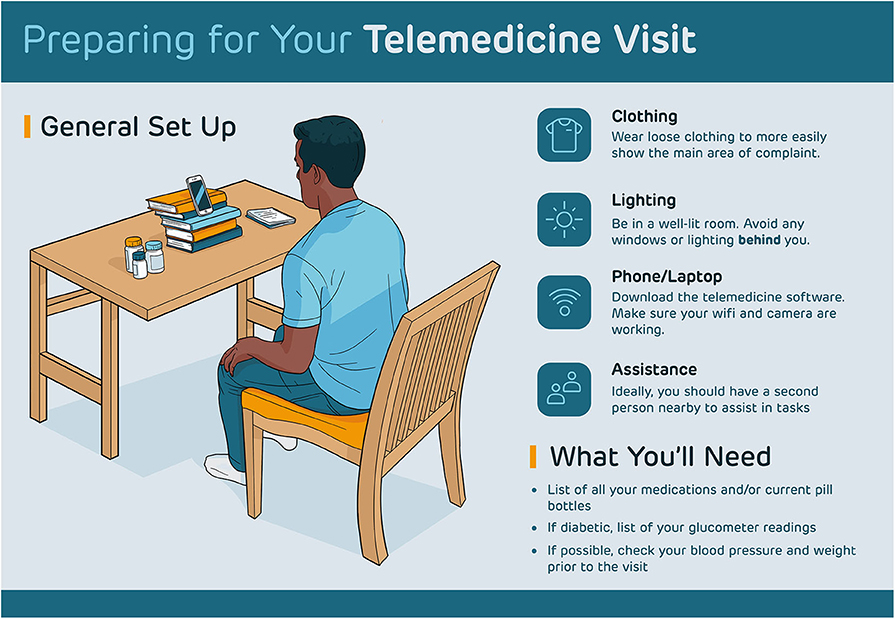
Tele-Health medical providers are cheering the Drug Enforcement Agency (DEA) move to temporarily extend virtual prescribing flexibility.
The DEA is looking to buy some time to consider whether it should require patients to see doctors face-to-face to get prescriptions for controlled drugs or continue to allow Tele-Health prescriptions. The agency received a record 38,000 public comments on its proposed rule.
Posted on September 20, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Jules Murtha
***
***
Here’s What Doctors Need to Know
The Supreme Court of the United States (SCOTUS) has ruled that doctors must show intent to mis-prescribe opioids in order to face criminal charges.
Despite the drop in opioid prescriptions in recent years, opioid overdoses and deaths are on the rise, largely because of street drugs.
The CDC’s position is that physicians can better serve patients by focusing on when to initiate and continue opioid treatment, what type and dosage of opioid to use, and how to address risk of drug abuse when prescribing opioids.
Posted on May 9, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Dr. David Edwarrd Marcinko MBA
Rx DRUG ABUSE
Traditional medicinal agents come in a variety of ways, known as dispensing vehicles. Drugs may be in liquid, pill or inject able form, they may be compounded in capsules, caplets, gelatin tablets, powders or suppositories, or they may come in creams or ointments for the eye, anus and vagina. They may be ingested into the stomach, placed and dissolved under the tongue, put into the eyes, popped, injected or smeared and transported through the human skin from patches.
A valid drug prescription is a written order, by a doctor, to a pharmacist. In this country, prescriptions are written by physicians, podiatrists, osteopaths, dentists. and some optometrists, physician assistants and nurse practitioners. In addition to the name of the patient and that of the medical prescriber, the prescription contains the name of the drug (not necessarily a narcotic), its quantity, instructions to the pharmacist, and directions to the patient. Narcotic prescriptions may not be prescribed to a drug addict to prevent withdrawal symptoms, as there must be some other therapeutic purpose for such an order.
The art of medicinal prescription writing, and pharmaceutical compounding, has declined in modern medicine for several reasons. Most drugs are made by pharmaceutical companies, and the role of the pharmacist, in most cases, consists only of compounding and error prevention. Many drugs are even automatically dispensed, and tracked, in the hospital setting with bar coding technology and modern inventory tracking mechanisms. Also, the practice of writing long and complicated prescriptions, containing many active ingredients, adjuvants, correctives, and elegant vehicles, has been abandoned in favor of using pure compounds.
Drugs may be prescribed by their official names, which were first given by the United States Pharmacopeia (USP), in 1920, or by the National Formulary (NF), since 1906. Unofficial or generic names may be used, known as New and Non-Official Drugs (NND) or by the United States Adopted Names (USAN), or by the manufactures trade name. For example, the generic narcotic meperidine or pithidine, is also known by the trade named, demerol. The designation USAN does not imply endorsement by the American Medical Association (AMA) Council on Drugs (CODs), or by the USP.
Of course, there is an advantage and disadvantages to prescribing drugs by their trade name, or generic names. Advantages of generics include economies of scale for both the patient and pharmacist, and although the active ingredient in generics are identical to trade drugs, they are often less expensive since research and development costs are absent, and various binders, colorizing agents, preservatives or dispersing agents are of an inferior quality, and hence cheaper for the patient. Appearance, size and taste issues are common. For the pharmacist, generics are cheaper since a multiplicity of very similar drugs need not be shelved.
***
***
For example, the tablet or capsular form of many drugs contains inactive ingredients, such as: ammonio methacrylate copolymer, hydroxypropyl methylcellulose, lactose, magnesium stearate, povidone, redironoxide, stearyl alcohol, talc, titanium dioxide, triacetin, yellowironoxide, yellowironoxide with FD&C blue No.2 (80 mgstrengthtablet only), FD&C blue No.2 and other ingredients. And yes, I’ve seen an addict do into shock, or die from acute anaphylaxis, after taking drugs containing ingredient he was highly allergic to.
Shock is a life-threatening condition where blood pressure falls too low to sustain life. It occurs when low blood volume (due to severe bleeding, excessive fluid loss or inadequate fluid uptake), inadequate pumping action of the heart or excessive dilation of the blood vessel walls (vasodilation) causes low blood pressure. This in turn results in inadequate blood supply to body cells, which can quickly die or be irreversibly damaged.
Anaphylactic shock is the severest form of allergy that is a medical emergency. It is a Type I reaction according to the Gell and Coombs medical classification, and is often severe and sometimes fatal systemic reaction in a susceptible individual upon exposure to a specific antigen (such as wasp venom or penicillin) following previous sensitization, or drug use. Characterized especially by respiratory symptoms, fainting, itching, itching and swelling of the throat or other mucous membranes and a sudden decline in blood pressure! The victim literally cannot breathe and drowns in its own congested and fluid filled lungs
So, patients in need of routine drugs for acute or chronic conditions like arthritis, high blood pressure, asthma, acne, hay fever, performance enhancing steroids or, so called life style drugs, like Viagra for a limp woody, or hair growth stimulator Rogaine, may get a good deal by going to Canada or Mexico for generics. But for important drugs, like nitroglycerine fro your heart, blood thinner coumadin, birth control pills or various anti-cancer agents, stick with brand names.
The main disadvantage of trade drugs is increased cost, due to R & D, patents, trademarks, marketing and company advertising expenses. Of course, trade drug are first to market, and hence may be beneficial as a new treatment modality, or injurious if significant side affects or other complications arise.
Today, the prime source for drug information is probably the well known, Physicians Desk Reference (PDR). Now, in its 58th edition, the PDR® provides the latest information on prescription, but not illegal street drugs. It is considered the standard reference that can be found in virtually every physician’s office, hospital and pharmacy in the United States. The current edition is over 3,000 pages long, and is where you can find data on more than 4,000 drugs, by brand and generic name, manufacturer and product categories. The PDR also provides usage information and warnings, drug interactions, plus full-size, full-color photos cross-referenced to specific drugs. For the layman, it also includes: phonetic spelling for each listing, a key to controlled substances, adverse reactions and contraindications, pregnancy ratings, dosages and all other FDA-required information. Of course, on the street, or in Mexico, none of this information matters.
Latin abbreviations, sometimes still used by doctors on prescription blanks include:
Rx = take thou (receipe)
po = by mouth (para orbis)
prn = as needed (pro re’nata)
hs = at bed time (hora somnae)
BID = twice daily
TID = three times daily
QID = four times daily
M = Mix
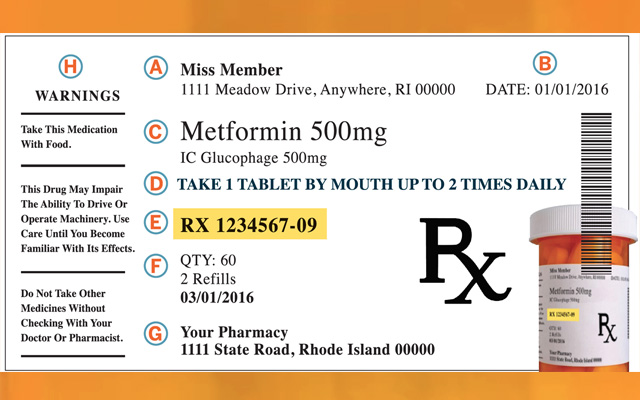
Traditionally, a medical prescription is written in a certain order, well known to drug abusers, and DEA agents, and consist of six basic parts:
Superscription: This is the Rx, or recipe. In Latin it means take thou.
Inscription: Represents the ingredients and amounts.
Subscription: Represent the description for drug dispensing, and may be represented by the letter M, for mix.
Signature: Often abbreviated as Sig, and contains the directions for patient use.
Refill Status: Indicates the number of refills allowed.
DEA Number: This is nine-character alpha-numeric sequence, used by all licensed physicians who prescribe narcotic agents. An example is AM2685591. The second letter is the first letter of the doctor’s last name, (ie, Marcinko) and the first two digits add up to the third (ie, 2+6=8).
Finally, in addition to the basic parts of a prescription, it should have the patient’s name, and physician signature written in ink, followed by degree designation, such as MD, DPM, DO or DDS, etc.
***
***
Perhaps the most egregious narcotic prescribing habits recently encountered by DEA agents have been by doctors of all degrees and medical designations. Reasons are generally two-fold. First, the doctor may become a drug addict himself, either by accident or through initial legitimate therapeutic use, and over-prescribe the narcotics. Or, increasing office costs, and decreased reimbursement fee reductions of many managed medical care have so economically destabilized the medical community, that economically impoverished doctors desperately sell prescriptions to finance their personal lifestyles, automobiles, clothes, fancy vacations or own addictions.
For example, a staggering medical student loan debt burden of $100,000-$250,000 is not unusual for new practitioners. In fact, the federal Health Education Assistance Loan (HEAL) program reported that for the Year 2001, it squeezed significant repayment settlements from its Top 5 list of deadbeat doctor debtors. This included a $303,000 settlement from a New York dentist, $186,000 from a Florida osteopath, $158,000 from a New Jersey podiatrist, $128,000 from a Virginia podiatrist, and $120 from a Virginia dentist. The agency also excluded 303 practitioners from Medicare, Medicaid and other federal healthcare programs and had their cases referred for non-payment of debt.
These facts indicate that the current healthcare reimbursement climate has caused more pain and tumult to doctors than the pubic realizes. Older medical practitioners are retiring prematurely, mature providers are frustrated and in despair, and young physicians have no concept of the economic servitude to which they are about to be subjected. Frustration is high and physician suicides have been documented. Many doctors get divorced at the start of their careers. Even the U.S. Inspector General has declared healthcare providers to be public enemy #2,behind international narco-traffickers, for their federal drug, fraud and abuse initiatives. Still, the statistic above lends itself to narcotic drug prescription abuse, either on the part of the doctor or patient, since only these two parties that can directly alter a prescription for illicit drug use, as illustrated by this poorly written prescription for a narcotic pain killer, vicodin.
Posted on April 24, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
According to FOX News, a New York physician was charged in an unsealed indictment on Thursday over an alleged $10 million health care fraud scheme. The Department of Justice announced that Elemer Raffai, 56, was charged with health care fraud for his alleged involvement in an alleged scheme between July 2016 and June 2017, signing prescriptions and other order forms for services that weren’t medically necessary, the Department of Justice states.
Raffai allegedly signed prescriptions and other order forms through telemedicine services for durable medical equipment that the Department of Justice claims were not medically necessary.
Justice says that Raffai was partially convinced to make the prescriptions and orders due by the payments of bribes and kickbacks. The indictment also alleges that Raffai and other individuals either submitted or caused $10 million in false and fraudulent claims to be submitted to Medicare, which paid more than $4 million on the claims.
If convicted, the physician faces a maximum of 10 years in prison
Posted on March 15, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
****
54% of Pharmacists Lack Time to Complete Their Job Effectively
According to the “2022 Medication Access Report“:
• 54% of pharmacists said they lack time to complete their job effectively. • Of the 54%, 81% cited inadequate staffing and 73% cited time-consuming administrative tasks. • Physicians felt strained by unprecedented demands, with 42% reporting burnout and 69% feeling depressed.
Posted on January 25, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
StockMarkets: The major equity indexes staged a thrilling comeback to close solidly in positive territory. At one point, the NASDAQ was down nearly 5% and the S&P entered correction territory.
Mark Cuban: The billionaire owner of the Dallas Mavericks just launched an online pharmacy for generic drugs that looks to cut out middlemen and combat pharmaceutical industry price gouging by offering steep discounts. Set up as CostPlusDrugs.com with 100 generic drugs to treat conditions like diabetes and asthma. Cost Plus will not accept health insurance but claims its prices will still be lower than what people would typically pay at a pharmacy. “All drugs are priced at cost plus 15%!” Cuban tweeted.
Posted on July 7, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
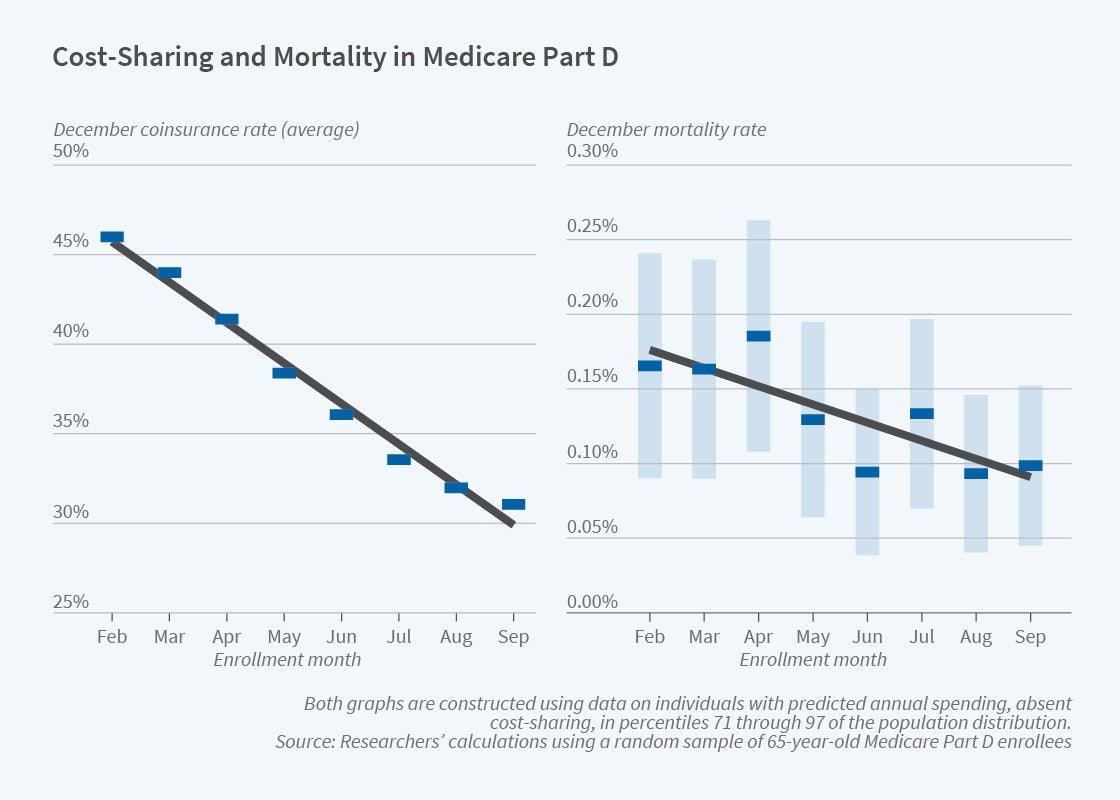
Raises Mortality among Medicare PART D Beneficiaries
QUERY: What are the health consequences when patients reduce their use of prescribed medications in response to higher out-of-pocket costs?
In The Health Costs of Cost-Sharing (NBER Working Paper 28439), researchers Amitabh Chandra, Evan Flack and Ziad Obermeyer use the distinctive out-of-pocket cost-sharing features of Medicare Part D to demonstrate that such reductions can increase mortality.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
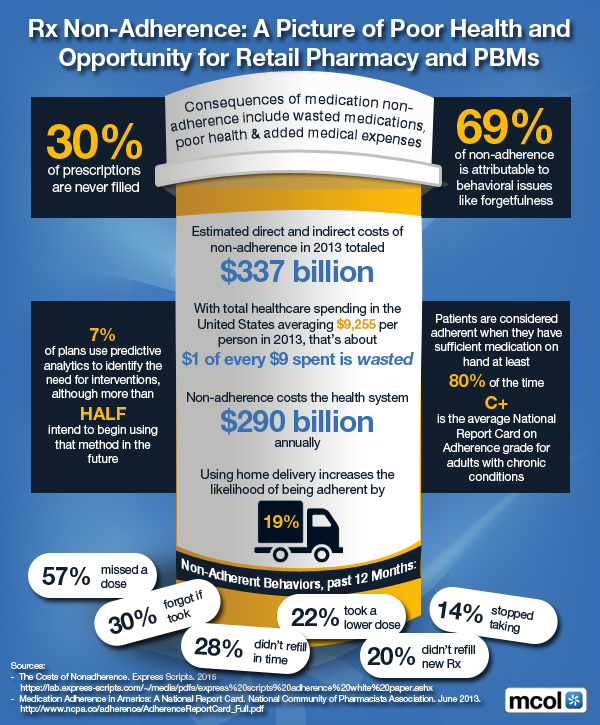
A Picture of Poor Health and Opportunity for Retail Pharmacy and Pharmacy Benefits Managers [PBMs]
***
***’
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Medicare’s popular prescription-drug program now serves more than 35 million people, but the names of prescribers and the drugs they choose have never previously been public … Until now.
###
Assessment
Use this tool to find and compare doctors and other top prescribers in 2010.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
****
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 17, 2012 by Dr. David Edward Marcinko MBA MEd CMP™
Spending expected to increase from 25 to 40 percent by2037
[By Staff Reporters]
Rising healthcare costs is exploding with the cost of healthcare currently outpacing inflation with federal health spending expecting to increase from 25 percent to 40 percent by 2037 equivalent to 25 percent of the American economy. With the country still in a recession and all the changes in healthcare reform has brought the issue as one of the hot topics for the fall’s presidential election.
Key Drivers of Rising Healthcare Costs
Hospital care and physician/clinical services combined account for half (51%) of the nation’s health expenditures sparking debates on how healthcare spending can be controlled. Some of the key drivers of rising healthcare costs are:
Prescription Drugs/Technology – Pharma is usually the biggest culprit associated with rising healthcare costs; however, medical technology has also been cited as a driver to an increase in overall healthcare spending. Cutting edge technology and drugs can fuel healthcare costs due to development costs and services.
Rise in Chronic Diseases – Baby boomers getting older, longer life spans, and the epidemic rates of obesity create an expensive dilemma for the healthcare system. Efforts have increased with the adoption of accountable care and healthcare technology to provide tools for chronic disease management while lowering costs.
Administrative Costs – 7% of health care expenditures are estimated to go toward for the administrative costs of government health care programs and the net cost of private insurance (e.g. administrative costs, reserves, taxes, profits/losses).
This infographic outlines several important statistics relevent to the healthcare spending debate including:
The U.S spends 2.5x more on healthcare per capita than other wealthy countries, but yet scores far below these same countries in average life expectancy.
The growth rate of healthcare spending far exceeds the growth of our national economy and wages
On average, current healthcare premiums cost the American family 16% of their gross income.
A Few Queries to Consider
How will ACA affect healthcare spending?
Can the adoption of Health IT (e.g. chronic disease management tools, patient remote monitoring, mobile health, and others) improve quality of care without increasing healthcare spending?
What role should individual states play in controlling costs?
How do we effectively address the low income families?
Assessment
This Infographic highlighted the rising healthcare costs and what could be bought with the $2.8 trillion dollars that Americans spend on healthcare yearly.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The use of controlled substances in medicine is a heavily argued topic, with benefits being weighed heavily against the potential for abuse. So, today we’re taking a look at one side of the argument, namely the medical benefits and clinical uses of abused drugs. Please enjoy.
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Please review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on January 19, 2012 by Dr. David Edward Marcinko MBA MEd CMP™
An Infographic
This ME-P comes to us from Appature, a Seattle based company that provides a cloud based healthcare marketing tool.
Upon submission of this infographic, the folks at Appature had the following to say:
Appature Inc, a Seattle-based software company that makes marketing tools for the healthcare industry, just launched its first infographic about Prescriptions Most Marketed to Doctors in the healthcare industry! Our infographic breaks down the ins and outs of which prescriptions are most marketed to doctors, to which prescriptions have the greatest sales ($5.3 Billion!) and even patient sentiments regarding a doctor’s prescribing habits. By reading this infographic, we hope that readers will get a little peek inside the intricate inner-workings of the infamous pharmaceutical industry! As TIME magazine highlights, “…the pharmaceutical industry is – and has been for years – the most profitable of all businesses in the U .S.”
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES: