BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on November 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters and Copilot A.I.
***
***
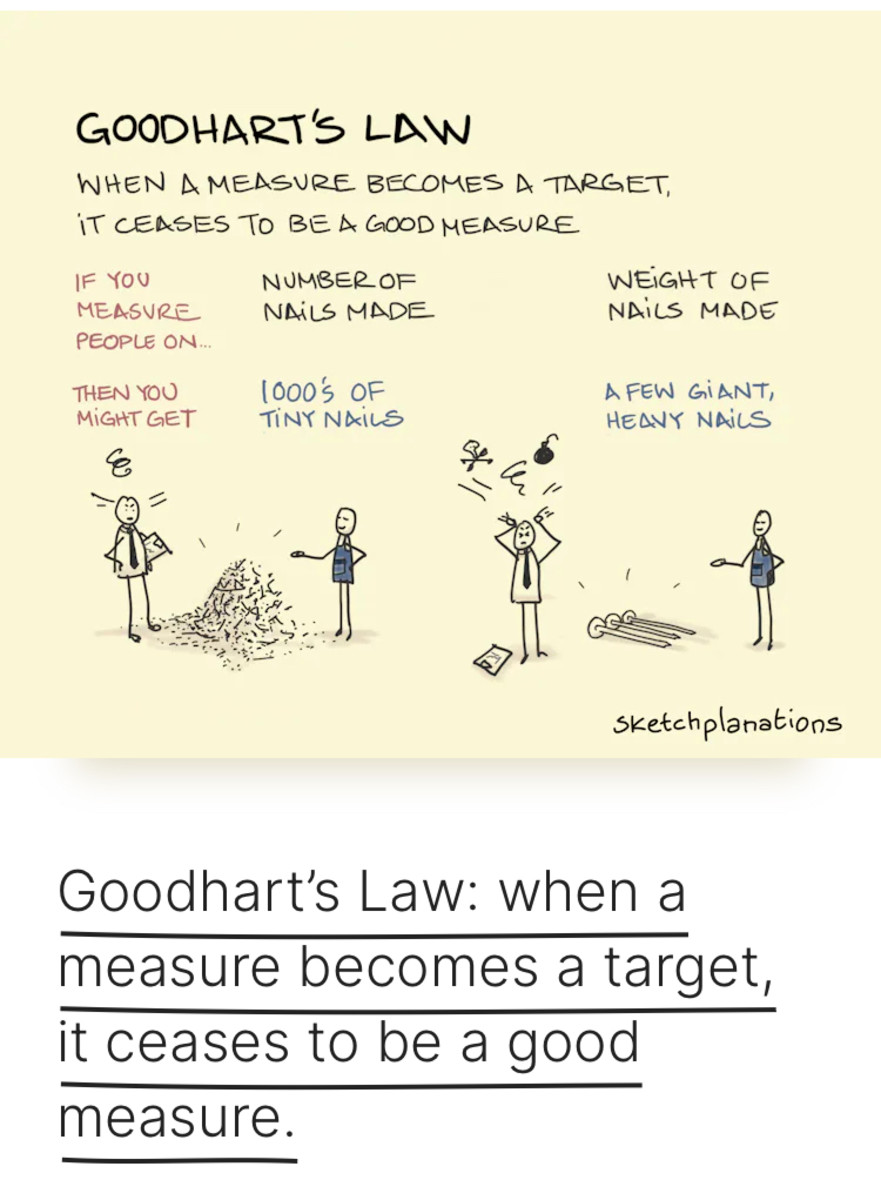
Goodhart’s law is an adage often stated as, “When a measure becomes a target, it ceases to be a good measure”. It is named after British economistCharles Goodhart, who is credited with expressing the core idea of the adage in a 1975 article on monetary policy in the United Kingdom:
Any observed statistical regularity will tend to collapse once pressure is placed upon it for control purposes.
It was used to criticize the British Margaret Thatcher Government for trying to conduct monetary policy on the basis of targets for broad and narrow money, but the law reflects a much more general phenomenon.
And so, aother famous Goodhart’s Law example is the cobra effect, where well-intentioned government policies inadvertently worsened the problem they were designed to solve.
For example, the British colonial government in India, concerned about the increasing number of venomous cobras in Delhi, began offering a bounty for each dead cobra that was delivered. Initially, this strategy was successful as locals brought in large numbers of slaughtered snakes. Over time, however, enterprising individuals started breeding cobras to kill them for supplemental income. When the government abandoned the bounty, the cobra breeders released their cobras into the wild, leading to a surge in Delhi’s snake population.
The cobra effect, where efforts to control a problem lead to unintended and often worse outcomes, serves as a cautionary tale for health care AI. If developers or health care institutions focus too narrowly on specific performance AI metrics, they risk undermining the system’s overall effectiveness, leading to suboptimal patient outcomes. Physicians must be vigilant in ensuring that health care AI systems are not only optimized for performance metrics but are also truly beneficial in practical, clinical applications.
Posted on September 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Authentication:
The verification of the identity of an individual, system, machine, or any other unique entity
Authorization:
The process of allowing access to specific areas of a system based on the role and needs of the user
Committee Charter:
A document that defines the purposes and responsibilities of the oversight committee
Compliance Risk Profile:
The current and prospective risk to earnings or capital arising from violations of or nonconformance with laws, rules, regulations, prescribed practices, internal policies and procedures, or ethical standards
Control Assessment:
A high-level review and analysis of controls relating to a process; should encompass both current and missing controls
Controls:
Methods that preserve the integrity of important information, meet operational or financial targets, and/or communicate management policies (See also: Key Control, Secondary Control, Tertiary Control)
ERM Policy Statement:
Defines an organization’s approach to and method of enterprise risk management
Governance:
Processes and structures implemented to communicate, manage, and monitor organizational activities
Impact:
The influence and effect of a risk
Inherent Risk:
Risk that is inherent to a process, taking into consideration the likelihood and impact of a risk
Key Control:
A primary control that is essential for a business process; typically takes place during the process it applies to
Key Indicators:
Measurements that are important for organizations to monitor for potential issues; examples include key performance indicators (KPIs) and key risk indicators (KRIs)
Key Performance Indicator (KPI):
A measurement with a defined set of goals and tolerances that gauges the performance of an important business activity
Key Risk Indicator (KRI):
A proactive measurement for future and emerging risks that indicates the possibility of an event that adversely affects business activities
Likelihood:
The probability of a risk occurring
Mitigation Actions:
The necessary steps, or action items, to reduce the likelihood and/or impact of a potential risk
Operation Risk Profile:
1) The risk arising from the execution of an organization’s business processes; 2) The risk of loss resulting from failed or inadequate internal processes, systems, people, or other entities
Price Risk Profile:
The risk to earning or capital arising from adverse changes in portfolio values
Process:
1) The principle elements of essential business functions within work groups or business units; 2) A set of tasks completed by business continuity plan owners within a department
Reputation Risk Profile:
The current and prospective risk to earnings or capital arising from negative public opinion or perception
Residual Risk:
Risk remaining after considering the existing control environment
Risk:
A potential event or action that would have an adverse effect on the organization
Risk Appetite:
A statement that broadly considers the risk levels that management deems acceptable
Risk Assessment:
The prioritization of potential business disruptions based on the impact and likelihood of occurrence; includes an analysis of threats based on the impact to the organization, its customers, and financial markets
Risk Tolerance:
A metric that sets the acceptable level of variation around organizational objectives and provides assurance that the organization remains within its risk appetite
Secondary Control:
An important control that typically takes place after the process it applies to (i.e., reporting or ongoing monitoring)
Strategic Risk Profile:
The current and prospective risk to earnings or capital raising from adverse business decisions, improperly implemented decisions, or lack of responsiveness to industry changes
Tertiary Control:
A non-essential control that can still be applied effectively to a business process
Velocity:
The time it takes a risk event to manifest itself
Vulnerability:
An entity’s susceptibility to a risk event as determined by the entity’s preparedness, agility, and adaptability
Posted on August 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
LEADERSHIP versus MANAGEMENT
***
***
By Dr. David Edward Marcinko MBA MEd
By Professor Gary A. Cook PhD
By Professor Eugene Schmuckler PhD MBA MEd CTS
Many of us have encountered a person who may intellectually be at upper levels, but whose ability to interact with others appears to that of one who is highly immature. This is the individual who is prone to becoming angry easily, verbally attacks co-workers, is perceived as lacking in compassion and empathy, and cannot understand why it is difficult to get others to cooperate with them and their agendas.
THINK: Sheldon Cooper PhD D.Sc MA BA of the The Big Bank Theory TV show.
The concept of Emotional Intelligence [EQ] was brought into the public domain when Daniel Goleman authored a book entitled, Emotional Intelligence.” According to Goleman, emotional intelligence consists of four basic non-cognitive competencies: self awareness, social awareness, self management and social skills. These are skills which influence the manner in which people handle themselves and their relationships with others. Goleman’s position was that these competencies play a bigger role than cognitive intelligence in determining success in life and in the workplace. He and others contend that emotional intelligence involves abilities that may be categorized into five domains:
Self awareness: Observing and recognizing a feeling as it happens.
Managing emotions: Handling feelings so that they are appropriate; realizing what is behind a feeling; finding ways to handle fears and anxieties, anger and sadness.
Motivating oneself; Channeling emotions in the service of a goal; emotional self control; delaying gratification and stifling impulses.
Empathy: Sensitivity to others’ feelings and concerns and taking their perspective appreciating the differences in how people feel about things.
Handling relationships: Managing emotions in others; social competence & social skills.
In 1995, Goleman then expanded on the works of Howard Gardner, Peter Salovey and John Mayer. He further defined Emotional Intelligence as a set of competencies demonstrating the ability one has to recognize his or her behaviors, moods and impulses and to manage them best, according to the situation. Mike Poskey, in “The Importance of Emotional Intelligence in the Workplace.” continued this definition by stating that emotional intelligence is considered to involve emotional empathy; attention to, and discrimination of one’s emotions; accurate recognition of one’s own and others’ moods; mood management or control over emotions; response with appropriate emotions and behaviors in various life situations (especially to stress and difficult situations); and balancing of honest expression of emotions against courtesy, consideration, and respect.
Source: Emotional Intelligence: what is and why it matters” – Cary Cherniss, PhD, presented at the annual conference of the Society of Industrial and Organizational Psychology, April 2000.
EQ differs from what has generally been considered intelligence which is described in terms of one’s IQ.
Traditional views of intelligence focused on cognition, memory and problem solving. Even today individuals are evaluated on the basis of cognitive skills. Entrance tests for medical, law, business, undergraduate and graduate schools base admissions in large part on the scores of the SAT, GMAT, LSAT, MCAT, etc. Without question, cognitive ability is critical but has been demonstrated, it is not a very good predictor of future direct job performance and indirect liability management. In fact, in 1940, David Wechsler the developer of a widely used intelligence test made reference to “non-intellective” elements. By this Wechsler meant affective, personal and social factors.
Source: Non-Intellective factors in intelligence. Psychological Bulletin, 37, 444-445.
Goleman became aware of the work of Salovey and Mayer having trained under David McClelland and was influenced by McClelland’s concern with how little traditional tests of cognitive intelligence predicted success in life. In fact, a study of 80 PhDs in science underwent a battery of personality tests, IQ tests and interviews in the 1950s while they were graduate students at Berkeley. Forty years later they were re-evaluated and it turned out that social and emotional abilities were four times more important than IQ in determining professional success and prestige.
Source: Feist & Barron: Emotional Intelligence and academic intelligence in career and life success. Paper presented at the Annual Convention of the American Psychological Society, San Francisco, 1996.
Undoubtedly, we want to have individuals work with us who have persistence which enables to them have the energy, drive, and thick skin to develop and close new business, or to work with the patients and other members of the staff. It is important to note that working alongside one with a “good” personality may be fun, energetic, and outgoing.
However, a “good personality does not necessarily equate to success. An individual with a high EQ can manage his or her own impulses, communicate effectively, manage change well, solve problems, and use humor to build rapport in tense situations. This clarity in thinking and composure in stressful and chaotic situations is what separates top performers from weak performers.
Poskey outlined a set of five emotional intelligence competencies that have proven to contribute more to workplace achievement than technical skills, cognitive ability, and standard personality traits combined.
***
***
A. Social Competencies: Competencies that Determine How We Handle Relationships
Intuition and Empathy – Our awareness of others’ feelings, needs, and concern. He suggested that this competency is important in the workplace for the following reasons:
Understanding others: an intuitive sense of others’ feelings and perspectives, and showing an active interest in their concerns and interests
Patient service orientation: the ability to anticipate, recognize and meet customer’s’ (patients) needs
People development: ability to sense what others need in order to grow, develop, and master their strengths
Leveraging diversity: cultivating opportunities through diverse people.
B. Political Acumen and Social Skills: Our adeptness at inducing desirable responses in others. This competency is important for the following reasons:
Influencing: using effective tactics and techniques for persuasion and desired results.
Communication: sending clear and convincing messages that are understood by others
Leadership: inspiring and guiding groups of people
Change catalyst: initiating and/or managing change in the workplace
Conflict resolution: negotiating and resolving disagreements with people
Collaboration and cooperation: working with coworkers and business partners toward shared goals
Team capabilities: creating group synergy in pursuing collective goals.
C. Personal Competencies: Competencies that determine how we manage ourselves
D. Self Awareness: Knowing out internal states, preferences, resources, and intuitions. This competency is important for the following reasons.
Emotional awareness: recognizing one’s emotions and their effects and impact on those around us
Accurate self-assessment: knowing one’s strengths and limits
Self-confidence: certainty about one’s self worth and capabilities
Self-Regulation: managing one’s internal states, impulses, and resources. This competency is important in the workplace for the following reasons.
Self-control: managing disruptive emotions and impulses
Trustworthiness: maintaining standards of honesty and integrity
Conscientiousness: taking responsibility and being accountable for personal performance
Adaptability: flexibility in handling change
Innovation: being comfortable with an openness to novel ideas, approaches, and new information.
E. Self-Expectations and Motivation: Emotional tendencies that guide or facilitate reaching goals. This competency is important in the workplace for the following reasons.
Achievement drive: striving to improve or meet a standard of excellence we impose on ourselves
Commitment: aligning with the goals of the group or the organization
Initiative: readiness to act on opportunities without having to be told
Optimism: Persistence in pursuing goals despite obstacles and setbacks
A note of caution is necessary. Goleman and Salovey both stated that emotional intelligence on its own is not a strong predictor of job performance. Instead they contend that it provides the bedrock for competencies that are predictors.
Obviously, EQ is an important attribute and it behooves each of us to promote emotional intelligence in the workplace. A number of guidelines have been developed for the Consortium for Research on Emotional Intelligence in Organizations by Goleman and Cherniss. The guidelines cover 21 phases which include preparation, training, transfer and evaluation.
Assess the organization’s needs: Determine the competencies that are most critical for effective job performance in a particular type of job. In doing so, us a valid method, such as the comparison of the behavioral interviews of superior performs and average performers. Also make sure the competencies to be developed are congruent with the organization’s culture and overall strategy.
Assess the individual: This assessment should be based on the key competencies needed for a particular job, and the data should come from multiple sources using multiple methods to maximize credibility and validity.
Deliver assessments with care: Give the individual information on his/her strengths and weaknesses. In doing so, try to be accurate and clear. Also, allow plenty of time for the person to digest and integrate the information. Provide feedback in a safe and supportive environment in order to minimize resistance and defensiveness. Avoid making excuses or downplaying the seriousness of deficiencies.
Maximize choice: People are motivated to change when they freely choose to do so. As much as possible, allow people to decide whether or not they will participate in the development process, and have them change goals themselves.
Encourage people to participate: People will be more likely to participate in development efforts if they perceive them to be worthwhile and effective. Organizational policies and procedures should encourage people to participate in development activity, and supervisors should provide encouragement and the necessary support. Motivation will be enhanced if people trust the credibility of those who encourage them to undertake the training.
Link learning goals to personal values: People are most motivated to pursue change that fits with their values and hopes. If a change matters little to people, they won’t pursue it. Help people understand whether a given change fits with what matters most to them.
Adjust expectations: Builds positive expectations by showing learners that social and emotional competence can be improved and that such improvement will lead to valued outcomes. Also, make sure that the learner has a realistic expectation of what the training process will involve.
Gauge readiness: Assess whether the individual is ready for training. If the person is not ready because of insufficient motivation or other reasons, make readiness the focus of intervention efforts.
Foster a positive relationship between the trainers and learners: Trainers who are warm, genuine, and empathic our best able to engage the learners in the change process. Select trainers who have these qualities, and make sure that they use them when working with the learners.
Make change self-directed: Learning is more effective when people direct their own learning program, tailoring it to their unique needs and circumstances. In addition to allowing people to set their own learning goals, let them continue to be in charge of their learning throughout the program, and tailor the training approach to the individual’s learning style.
Set clear goals: People need to be clear about what the competence is, how to acquire it, and how to show it on the job. Spell out the specific behaviors and skills that make up the target competence. Make sure that the goals are clear, specific, and optimally challenging.
Break goals into manageable steps: change. That is more likely to occur if the change process is divided into manageable steps. Encourage both trainers and trainees to avoid being overly ambitious.
Provide opportunities to practice: Lasting change requires sustained practice on the job and elsewhere in life. An automatic habit is being unlearned and different responses are replacing it. Use naturally occurring opportunities for practice at work, and in life. Encourage the trainees to try the new behaviors repeatedly and consistently over a period of months.
Give performance feedback: Ongoing feedback encourages people and direct change. Provide focused and sustained feedback as the learners practice new behaviors. Make sure that supervisors, peers, friends, family members-or some combination of these- give periodic feedback on progress.
Rely on experiential methods: Active, concrete, experiential methods tend to work best for learning social and emotional competencies. Development activities that engage all the senses and our dramatic and powerful can be especially effective.
Build in support: Change is facilitated through ongoing support of others who are going through similar changes. Programs should encourage the formation of groups where people give each other support, throughout the change effort. Coaches and mentors also can be valuable in helping support the desired change.
Use models: Use modern webinars, patient portals, live or videotaped models that clearly show how the competency can be used in realistic situations. Encourage learners to study, analyze, and emulate the models.
Enhance insight: Self-Awareness is the cornerstone of emotional and social competence. Help learners acquire greater understanding about how their thoughts, feelings, and behavior affect themselves and others.
Prevent relapse: Use relapse prevention, which helps people use lapses and mistakes as lessons to prepare themselves for further efforts.
Moreover:
Encourage use of skills on the job: Supervisors, peers and subordinates should reinforce and reward learners for using their new skills on the job. Coaches and mentors also can serve this function. Also, provide prompts and cues, such as through periodic follow-ups. Change also is more likely to indoor. When high status persons, such as supervisors and upper-level management model it.
Develop an organizational culture that supports learning: Change will be more enduring if the organization’s culture and tone support the change and offer a safe atmosphere for experimentation.
Finally, see if the development effort has lasting effects evaluated. When possible, find a true set of measures of the competence or skill, as shown on the job, before and after training, and also at least two months later. One-year follow-ups also are highly desirable. In addition to charting progress on the acquisition of competencies, also assess the impact on important job related outcomes, such as performance measures, and indicators of adjustments such as absenteeism, grievances, health status, etc.
Managers V. Leaders
These abilities are important for one to be successful as a manager and even more so as a leader, or physician executive. But, before we begin an examination of strategic leadership, it is necessary to make a deeper distinction between a manager and a leader. There are many different definitions as well as descriptions regarding leadership and management.
Many people talk as though leadership and management is the same thing. Fundamentally, they are quite different. Management focuses on work. We manage work activities such as money, time, paperwork, materials, equipment, and personnel, among other things. As can be found in any basic book on management, management focuses on planning, organizing, controlling, coordinating, budgeting, finance and money management as well as decision making. In effect, managers are generally those individuals who have been given their authority by virtue of their role. It is the function of a manager to ensure that the work gets done as well as to oversee the activities of others. In many healthcare organizations we find that those individuals elevated to a managerial position occur as a result of being a high performer on their previous assignment. A manager receives authority on the basis of role; while a leader’ authority is more innate in nature.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on May 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
While the healthcare industry has been dealing with high employee turnover since the start of the COVID-19 pandemic, that turnover was largely among clinical staff.
However, a recent survey found that significant healthcare leadership turnover may also be on the horizon. AMN Healthcare subsidiary B.E. Smith found that nearly half of healthcare executives plan to leave their organization in the next year.
This Health Capital Topics article reviews the survey and the reasons behind the intended exits. (Read more…)
[Human Nature, Medical and Financial Ethics and Modern Principles]
In any medical blog or investing treatise of gravitas, thoughts on human nature are usually placed at the end of the work, or an afterthought if included at all. However, we elected to prominently place this material as a stand alone feature. Why?
In the end, the success of any financial advisor or physician endeavor ultimately comes down to changing human behavior – helping a doctor/nurse/technician alter whatever s/he was doing toward something that will better allow them to avoid errors and pursue quality care and investing or practice management goals.
Yet, there is still remarkably little education or training for financial planners or medical professionals focused directly on motivation or change theory, in any related area except psychiatry/psychology or perhaps professional liability. Instead, doctors and advisors/planners are increasingly turning to professional consultants to learn best practices on how to help them actually make the behavioral changes necessary to achieve their medical quality improvement and client acquisition goals; as we attempt to answer these questions:
Are you and your medical practice, or financial advisory practice, ready for change?
How to transition from [traditional] solo practitioner B-models to modern forms?
What are leadership, management and governance?
In group practices, how is leadership shared?
What issues need be considered when hiring a financial planner or practice administrator or clinic CEO?
What is medical ethics and financial munificence? Why is it needed? How does it work?
What are the types of risk?
How are risks managed in the medical practice space or financial advisory eco-system?
In addition, medical and financial planning practitioners need to strive to avoid what Zenger and Folkman describe as the 10 most common leadership shortcomings based on a survey of 11,000 leaders. They include:
Lacks energy and enthusiasm
Accepts mediocre self performance
Lacks clear vision and direction
Poor judgment
Not collaboration
Not following standards
Resistant to new ideas
Doesn’t learn from mistakes
Lacks interpersonal skills
Fails to develop others.
Source: Zenger and Folkman: The Daily Stat: The 10 Most Common Failures of Business Leaders, Harvard Business Publishing, June 4, 2009.
Posted on April 14, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
Understanding the Difference
[By Dr. David Edward Marcinko MBA]
Many times, individuals will use the terms management and leadership synonymously. In actuality the terms have significantly different meanings.
For example, Warren Bennis describes the difference between managers and leaders as “Managers do things right, Leaders the right thing.”
Managers are those individuals who have as their primary function managing a team of people and their activities. In effect, managers are those who have been given their authority by the nature of their role and ensure that the work gets done by focusing on day to day tasks and their activities.
On other hand, a leader’s approach is generally innate in its approach. Good leadership skills are difficult to learn because they are far more behavioral in nature than those skills needed for management. Leaders are also very focused on change recognizing that continual improvement can be achieved in their people and their activities can be a great step towards continued success.
Training Camps
Perhaps some of the best training grounds for the development of leaders are the military. The Marine Corps slogan is “A Few Good Men” and the military academies at Annapolis (Navy), New London, Connecticut (Coast Guard), Colorado Springs (Air Force), and West Point (Army) all have as their main mission, the development of leaders.
This is done by a number of different techniques. At graduation, the new officers, regardless of the branch of service, have been taught, and more importantly, have internalized the following: communicate the missions, sensitivity matters, real respect is earned, trust and challenge your soldiers. It is due to these lessons that many graduates of the military academies go on to positions of leadership in the private sector as well as in government. Communicating the mission refers to conveying to those who work with us what are practice is hoping to accomplish and the role of each employee in achieving that goal. Given an understanding and awareness of the mission, when confronted with a barrier, employees are able to face hard problems when there is no well-defined approach by which to deal with them.
***
***
Sensitivity Does Matter
This is my area to improve; as I can be glib on occasion.
A leader treats each employee with respect and dignity, regardless of race, gender, cultural background or particular role they actually perform in the practice. Consider how many legal suits are filed against any type of organization, whether it is a medical practice or a large manufacturing facility due to perceived disparate treatment towards the employee based on race, religion, gender sexual preference or other non-work related issues.
Real respect is earned – Having initials after one’s name and the wearing of a lab coat does not automatically entitle an individual to respect. Formal authority has been found to be one of the least effective forms of influence. Only by earning the respect of your staff as well as your patients can you be sure that your intent will be carried out when you are not present. Setting the example in performance and conduct, rather than ‘do as I say, not as I do,” level of activity enables one to exert influence far greater than titles.
Trust and challenge your employees – How many times have practices sought to hire the best and brightest only to second guess the employee. Eric Schmidt, the CEO of Google, describes his management philosophy as having “… an employee base in which everybody is doing exactly what they want every day.” Obviously there are certain policies and procedures, but at the same time, the leader enables decision making to the lowest possible level. This also enables employees to question why certain policies and procedures are still being followed when more effective and efficient methods are available. (How the Army Prepared Me to Work at Google, Doug Raymond, Harvard Business)
The phrase “Physician, heal thyself” (Luke 4:23, King James Version) means that we have to attend to our own faults, in preference to pointing out the faults of others. The phrase alludes to the readiness of physicians to heal sickness in others while sometimes not being able or will to heal themselves.
By the same token, it now is necessary for us to learn how to manage ourselves. It suggests that physicians, while often being able to help the sick, cannot always do so, and when sick themselves are no better placed than anyone else (Gary Martin, phrases.org.uk/meanings/281850.html, 2010).
***
***
Self-Development
“We will have to learn how to develop ourselves. We will have to place ourselves outside the boundaries where we can make the greatest contribution. And we will have to stay mentally alert and engaged during a 50-year working life, which means knowing how and when to change the work we do” (Managing Oneself, Harvard Business Review – Jan. 2005 – pp 100-109, by Peter Drucker).
Although one’s IQ and certain personality characteristics are more or less innate and appear to remain stable over time there are individual capabilities that enable leadership and can be developed. Enhancement of these capabilities can lead to the individual being able to carry out the leadership tasks of setting direction, gaining commitment, and creating alignment. These capabilities include self-management capabilities, social capabilities and work facilitation capabilities.
***
***
Assessment
Without question, while it is possible to cram for at test and graduate at the top of one’s class, that does not assure leadership ability. We all know at least one person who scores at the highest levels on cognitive measures but would be incapable of pouring liquid out of a boot if the instructions were written on the heel.
So, here is my philosophy:
Leadership: By example and thru transparency with collaboration [Do the right thing]
Management: By walking-around thru tangible / intangible metrics [Doing things right].
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on July 13, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Leadership Concepts for Physicians and Healthcare CXOs
By Dr. David Edward Marcinko MBA
[Editor-in-Chief]
The toughest part of implementing any medical quality improvement program is changing the healthcare organization’s culture. The physician-executive or chief executive officer must be committed to change, not just give lip service to it. The core to TQM or, for that matter, any of the several new popular quality programs, like six-sigma, is the buy-in of senior management to change the culture of the practice organization to support the individual’s pursuit of quality.
Re-Frame the Situation
The cultural change requires a complete reorientation of job descriptions and duties. It requires a collaborative rather than an adversarial work force. The phrase, “it’s not my job,” cannot work in a quality healthcare environment. Medical quality programs cannot work where employees refuse to be “their brothers’ keepers.” This collaborative working system is difficult to implement, but not impossible to achieve. It involves certain basic changes to the traditional American work ethic of “rugged individualism.” It suggests that the individual employee must become a partner in the healthcare enterprise and be just as concerned about quality as the CEO. Quality really does become everybody’s business.
Assessment
Quality requires new thinking about the relationships that have traditionally existed between labor [nurses, therapists, assistants, and aides, etc] and management [physician-owner, CEO, clinic administrator, managers, etc]. It requires a new direction; a new partnership must be forged between management and the clinical floor, between management and administrative staff, and between line and staff management.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 4, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Tracking Claims, Real-World Solutions
Staff Reporters
Dear Subscribers
Next year is the deadline for all Medicare healthcare providers to enroll in the Recovery Audit Contractor program. Due to national implementation, the market has become flooded with products to track claims, provide easy audit solutions, as well as aggregate data to predict which claims are at risk for recoupment.
And so, we have been asked to help facilitate this survey.
Past Surveys
According to our past survey, over 90 percent of respondents listed claim denials as a major problem for them. The editorial staff of Healthcare Reimbursement Monitor wants to know what steps your organization is taking to ensure the protection of claims through our latest query Healthcare Leadership Survey: Tracking Claims, Real-World Solutions
Assessment
What impact has the RAC program had on your organization? Are claims tracking software a necessity for today’s healthcare business? What type of claims solution does your organization need?
The Survey
Please take a quick moment to complete the short survey to allow your colleagues insight into best practices and solutions you have experienced, or to warn the community of which tools are simply excess. Share your experiences with the community by participating in the survey.
Sincerely
Healthcare Reimbursement Monitor
Health Resources Publishing
1913 Atlantic Avenue, Suite 200, Manasquan, NJ 08736
phone: 800-516-4343
fax: 888-329-6242
Assessment
Channel Surfing
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on February 3, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Past versusPresent in the Health 2.0 Era
By Susan Bock; MAOM, SPHR
If you don’t know where you’re going, any road can take you there.
Hundreds, if not thousands, of books, articles and training materials have been published on leadership skills; far fewer for physicians of course; but the basics remain the same.
Self Help Proliferation
Why is there such a proliferation of paper devoted to this subject? Perhaps, it is due to the fact that business leadership today is ever so different from leadership of yesterday. Every aspect of leadership has been under intense scrutiny, by employees, industry experts, physician-executives and business gurus. Much like healthcare today, the very form of leadership is in a state of evolution – changing, modifying and redefining its core values. A multitude of leadership theories or models have been developed, revised, reviewed and assessed by the experts. What is needed, therefore, is an integration of several models specifically appropriate for today’s healthcare business environment and modern healthcare executive.
Yesterday’s Death Knoll for Medicine
Replication of the leadership skills of yesterday is the death knoll for business today; especially for the business of healthcare. Leadership is no longer based on managing, directing, or supervising [top-down or command and control model].As stated by James S. Doyle in his book The Business Coach [A Game Plan for the New Work Environment],
“Today’s employees … do not respond well to bosses. Quite simply, they have plenty of other options where they will be treated as full members of a team.”
Societal norms, generational beliefs and expanding diversity in healthcare are, in part, contributing to the new business environment. Likewise, medical leaders are required to respond, react and re-direct in the moment.
What Makes a Leader?
In a recent Harvard Business Review publication, “What Makes a Leader”, author Daniel Goleman says that the desired traits most often sited were intelligence, toughness, determination, and vision.A sufficient level of technical and analytical ability is even more essential now that we have moved into the new millennium.
However, the leadership skills of this era are placing much more emphasis on the so-called ‘soft skills’ or ‘emotional intelligence’ and this may very well be the key attribute that distinguishes outstanding healthcare leaders from those who are merely adequate.
Multi Generations
It is common to have three generations represented in any organization. We have the Baby-boomers, Gen X and now, Gen Y. The Baby Boomer generation is saying with some sadness, “It sure isn’t want it used to be!”, while Generation Xers are saying “It’s about time things changed!” and the latest generation to enter the medical workforce, Gen Y’s, are saying “Ready or not, we’re here”.
Each generation is extraordinarily complex, bringing various skills, expertise and expectations to the work environment. Determining the best methods to unite such diverse thinking is one of the many challenges faced by business leaders.
Assessment
Is it any wonder that many leaders in the Baby Boomer generation find themselves at a loss? The days of functional leadership are gone and suddenly, no one cares about the expertise of the Baby Boomers or how they climbed the corporate ladder, in medicine or elsewhere. The concept of ‘paying your dues’ is as foreign to the younger generations as is life without email, wikis or social networks. Still not convinced? Just think about the election of Barack Obama as 44th president of these United States. Leadership in the era of Health 2.0 is no longer about controlling or dictating with intense focus on the bottom line; it is about collaboration, empowerment and communication.
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. How does the digital generation change the leadership equation in healthcare today?
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Our Other Print Books and Related Information Sources:
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest E-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.