U.S. Hospitals Feeling the Pain of Physician Burnout [REPRINT]
Source: Reuters Health News via MDLinx [11/22/17]

Hospitals are just beginning to recognize the toll of burnout on their operations
Experts estimate, for example, that it can cost more than $1 million to recruit and train a replacement for a doctor who leaves because of burnout. But, as no broad calculation of burnout costs exists, Dr. Tait Shanafelt, a former Mayo Clinic researcher who became Stanford Medicine’s first chief physician wellness officer in September said Stanford, Harvard Business School, Mayo Clinic, and the American Medical Association (AMA) are working on that. They have put together a comprehensive estimate of the costs of burnout at the organizational and societal level, which has been submitted to a journal for review.
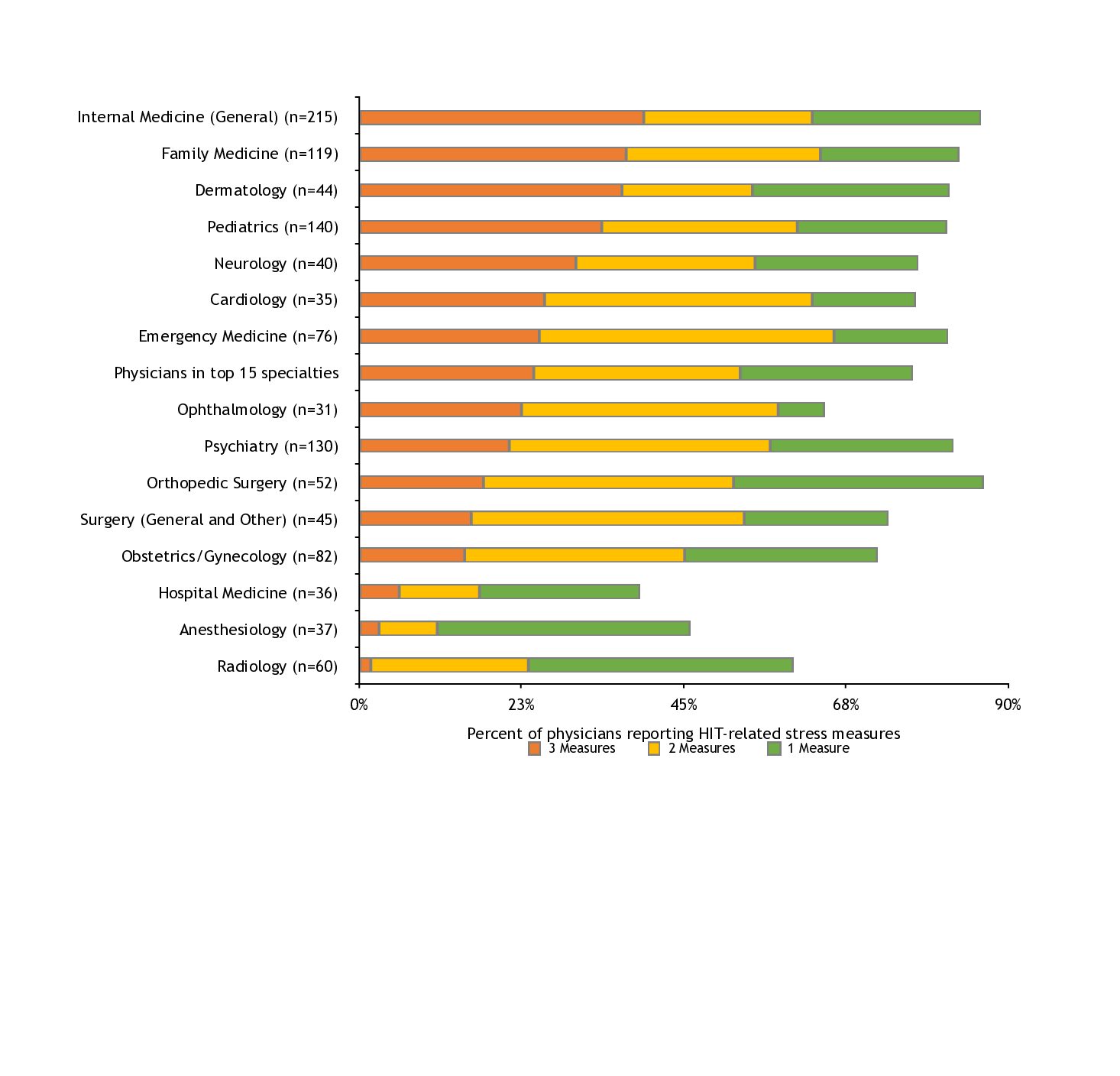
Shanafelt and other researchers have shown that burnout erodes job performance, increases medical errors, and leads doctors to leave a profession they once loved.
***

Hospitals can ill afford these added expenses in an era of tight margins, costly nursing shortages, and uncertainty over the fate of the Affordable Care Act, which has put capital projects and payment reform efforts on hold.
COACH
For a graphic, click here.
http://fingfx.thomsonreuters.com/gfx/rngs/TRAVIS%20HARTMAN/010051RR403/index.html
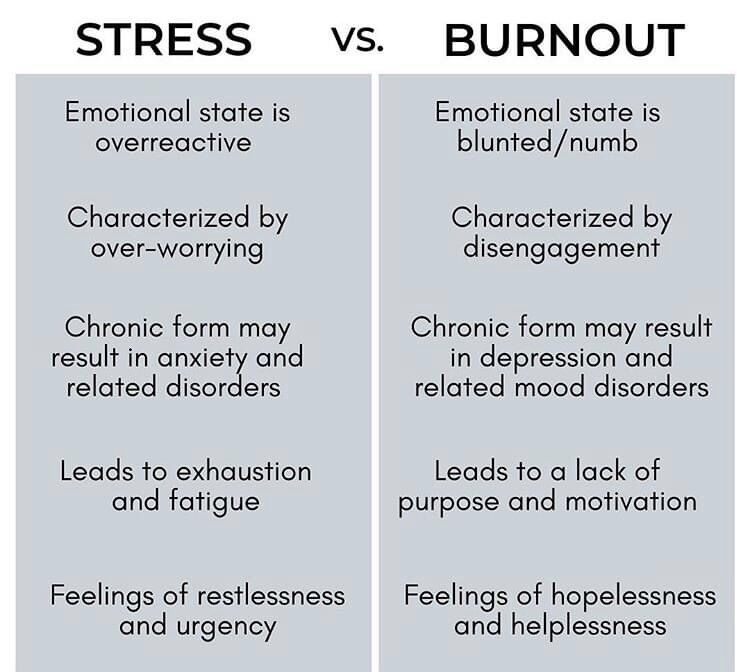
Sound familiar?
MORE
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
***


Filed under: Ethics, Practice Management | Tagged: Dr. Tait Shanafelt, Physician burnout | 5 Comments »














 ***
***



