











![]()
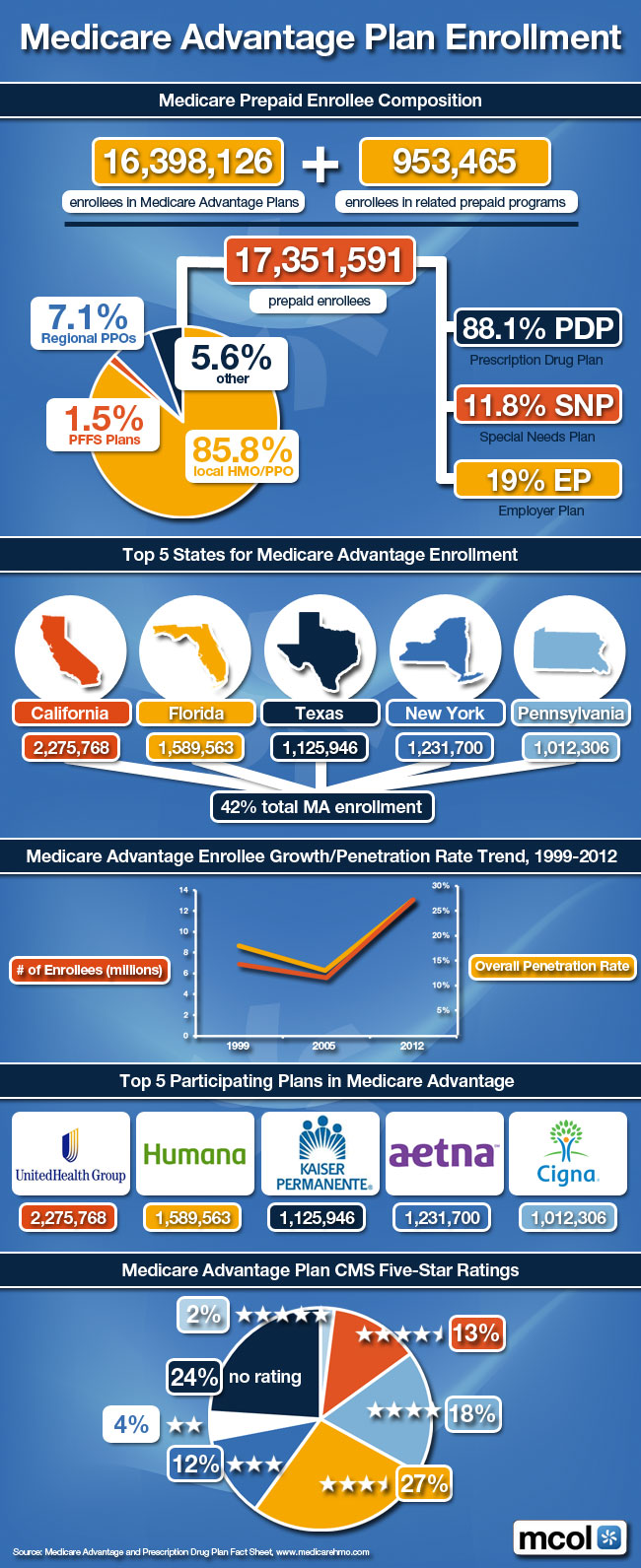
Medicare Pre-Paid Enrollee Composition
***
***
NOTE: CMS Releases 2013 Hospital, Physician Data
***
Source: Joseph Goedert, Health Data Management [6/2/15]
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
- PRACTICES: www.BusinessofMedicalPractice.com
- HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
- CLINICS: http://www.crcpress.com/product/isbn/9781439879900
- ADVISORS: www.CertifiedMedicalPlanner.org
- FINANCE: Financial Planning for Physicians and Advisors
- INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors
- Dictionary of Health Economics and Finance
- Dictionary of Health Information Technology and Security
- Dictionary of Health Insurance and Managed Care

![]()
Share this:

Filed under: Health Insurance | Tagged: medicare, Medicare Advantage, Medicare Advantage Plan, Medicare HMOs |

Big price hikes coming for Medicare premiums in 2016
Retirees, adjust your budget: Double-digit price hikes for Medicare Part B premiums are coming next year.
http://www.msn.com/en-us/money/insurance/big-price-hikes-coming-for-medicare-premiums-in-2016/ar-BBlH2oU?ocid=iehp
Amanda
LikeLike
Will the Silver Tsunami Send Medicare into the Red?
The youngest Baby Boomers will turn 65 in 2030—a demographic tsunami that will also see seniors living longer and with more disabilities and chronic illnesses.
These forces are driving projections that Medicare will become insolvent in 2030, barring substantial reforms. The program’s fiscal difficulties also stem from the fact the program’s beneficiaries typically reap far more in benefits than they’ve paid into the system.
Nancy Chockley PhD
LikeLike
CMS Proposes 1.35% Medicare Advantage Rate Hike for 2017
Baseline Medicare Advantage payment rates for 2017 will rise by 1.35% on average, an early win for health insurance companies in what is the final Medicare rate battle of the Obama administration. When factoring in the risk coding tendencies, the average change in Medicare Advantage insurers’ revenue will climb 3.55% next year, according to a CMS release posted late Friday. The proposal is a major shift from last February, when initial benchmark rates were cut by an average of 0.95% before factoring in risk score trends.
The 2017 proposal again makes changes to the program’s risk-adjustment model. Medicare Advantage insurers document the health status of their members by using risk scores that adjust for different demographics and conditions, known as hierarchical condition categories. A higher risk score indicates a person is sicker or has complicated chronic health conditions, which leads to a higher payment.
Source: Bob Herman, Modern Healthcare [2/19/16]
LikeLike
GAO confirms Center for Public Integrity’s findings on Medicare Advantage overspending
In a report last week, the U.S. Government Accountability Office confirmed what Fred Schulte and other journalists at the Center for Public Integrity (CPI) have been reporting on the Medicare Advantage program for two years…overspending.
Berl
LikeLike
23% of Medicare Advantage Plans Had Broad Hospital Networks in 2015
Kaiser Family Foundation recently released an analysis on Medical Advantage hospital networks. Here are some key findings from the report:
• Medicare Advantage plan networks included half (51%) of all hospitals in their county.
• 80% included an Academic Medical Center in their network, but 1 in 5 did not.
• 2 in 5 plans in areas with an NCI-designated cancer center did not include the center in their networks.
• 23% of Medicare Advantage plans in our study had broad hospital networks in 2015.
• 1 in 6 plans (16%) had narrow or ultra-narrow hospital networks in 2015.
• Among HMOs, broad and narrow network plans had similar average premiums ($37 vs. $36 per month).
Source: Kaiser Family Foundation, June 20, 2016
LikeLike
11% of Medicare Advantage Enrollees Voluntarily Switched Plans
Kaiser Family Foundation recently released an analysis on how often enrollees switch Medicare Advantage (MAPD) plans. Here are some key findings from the report:
• 11% of enrollees voluntarily switched Medicare Advantage plans for 2014.
• 8 in 10 enrollees stayed in the same plan from one year to the next.
• 4% were forced to switch because their plan exited the marketplace.
• MAPD enrollees who switched plans paid $17.51 less per month on premiums.
• The new plans had $401 lower out-of-pocket limits than the previous plans.
• 43% of ACA marketplace enrollees switched plans between 2015 and 2016.
Source: Kaiser Family Foundation, September 20, 2016
LikeLike
Medicare Advantage Premiums Will Drop 4% in 2017
Avalere recently released an analysis of data on premiums for stand-alone prescription drug plans (PDPs). Here are some key findings from the report:
• United is increasing premiums in AARP MedicareRx Preferred by about $10..
• In 2017, 678 PDPs will be offered, a 23% decrease from 886 in 2016.
• 88% of Part D Plans will have an average premium increase of 4% in 2017.
• The average MA premium will drop 4% in 2017, to $31.40.
• 78% of Medicare Advantage beneficiaries will have a $0 premium option in 2017
Source: Avalere, September 28, 2016
LikeLike
Medicare Advantage Risk Score Transition – RAPS to EDS Impact, Issues and Implications
Starting in 2008, CMS began the effort to transition from using Risk Adjustment Processing System (RAPS) data files to using Encounter Data System (EDS) data files as the basis for Medicare Advantage member risk scores. The shift to EDS data for calculating risk scores poses substantial financial risks for MAOs that are unprepared or ill-equipped to submit and monitor the EDS submissions. For many MAOs, risk-adjusted revenue makes up over 80% of total Medicare Advantage revenue. MAOs may be at significant financial risk if they have declines in risk scores and the revenue associated with their risk scores.
Milliman completed a study of how the transition from RAPS data to EDS data is affecting the payment year (PY) 2016 risk scores and revenue for Medicare Advantage. Fifteen MAOs participated in the study, reflecting a cross-section of small and medium size organizations and representing over 900,000 members in 154 plans. Study participants saw a median decrease in risk scores of 4% when comparing EDS scores with RAPS scores. 2017 mid-year risk score updates will be based only on RAPS (not on EDS, RAPS, and Medicare fee-for-service (FFS) claims).
MAOs have more time to review their EDS diagnosis submissions between now and May 1, 2017, in order to improve any deficiencies in their EDS submission processes. Despite revisions from CMS, these issues are not fully resolved. There are a number of steps MAOs should consider regarding their diagnosis submissions to address these issues.
Vera
LikeLike
Medicare Advantage Rip-Off
Private insurers rip off Medicare Advantage for billions
http://www.msn.com/en-us/money/healthcare/private-insurers-rip-off-medicare-advantage-for-billions/ar-BBBdfOJ?li=BBnb7Kz
Ruth
LikeLike
Medicare Advantage Beneficiaries Had 33% Fewer ER visits than FFS
Avalere recently published an analysis comparing Medicare Advantage (MA) to Fee-for-Service Medicare (FFS). Here are some key findings from the report.
• Medicare Advantage patients had 23% fewer hospitalizations than FFS Medicare.
• MA beneficiaries had 33% fewer emergency room visits than FFS beneficiaries.
• Annual spending/person on preventive services was 21% higher in Medicare Advantage.
• Medicare Advantage beneficiaries had a 57% higher rate of serious mental illness.
Source: Avalere, July 2018
LikeLike