![]()
Understanding the Referral Relationship
[By Dr. David Edward Marcinko MBA]
 Developing and cultivating a steady stream of referrals involves good planning, an investment of time and energy in the referral relationship, and a keen understanding of referring physicians’ needs and priorities.
Developing and cultivating a steady stream of referrals involves good planning, an investment of time and energy in the referral relationship, and a keen understanding of referring physicians’ needs and priorities.
Enhancing the referral relationship is a step-by-step process, not unlike the clinical process, that begins by identifying target physicians and their needs, prioritizing the list of referral contacts and then determining the best way to reach them.
A physician may routinely refer patients to a particular specialist because he or she has an outstanding reputation for medical expertise and competence, is more accessible than comparable practitioners or has a convenient location for the referring physician’s patients. The physician may have a relationship with the specialist because of marketing by a local hospital or the specialist’s own practice. And, in some cases the two physicians have a social relationship. Once again, there are many ways to create and maintain the relationship. Physicians should choose the approach that works best for them, put together a plan and stay consistent. Look for ways to make the relationship a win-win for both practices or for the referring hospital or outpatient facility.
If you are not comfortable with developing referral relationships for your practice, seek out partners, office staff or hospital partners who can appropriately assist, train or support you in this effort. Many hospitals have staff focused on physician sales and service.
The Society for Healthcare Strategy and Market Development (SHSMD) recently reported that 41% of hospitals had dedicated sales staff support, with more than half of those using their sales staff to support cardiology and radiology.[i] Often, hospitals are seeking physician speakers for community seminars, wellness programs and other outreach efforts. Ask about participating in these venues. Offer to write articles for newsletters, the Web site or local media outlets. All of these expose the physician and the practice to referral sources as well as the public.
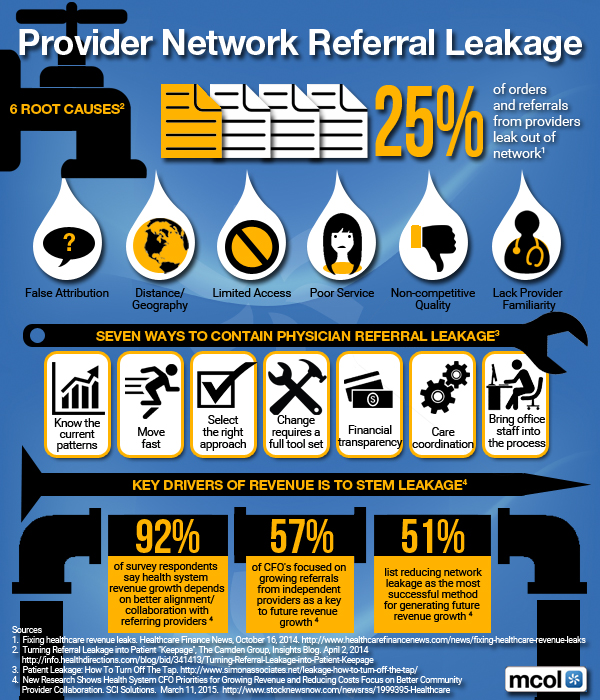
Six Root Causes of Leakage
***
***
Communication is Key
It really comes down to the age-old golden rule of doing unto others as you would want them to do unto you. Not surprisingly, referral relationships are built on mutual respect, trust and courtesy. Focusing on the needs of the referring physician is the best way for both relationships to thrive.
Communication is especially important in not only nurturing the referral relationship, but also improving the quality of care.
A recent study that examines the attitudes primary care physicians have regarding communication with hospitalists found that 3% of primary care physicians reported being involved in discussions about discharge and 17% to 20% reported always being notified about discharges.[ii]
The study suggests that delayed or inaccurate communication at discharge may negatively effect continuity of care and contribute to adverse events. Communication tools such as computer-generated summaries and standardized formats may result in a more timely transfer of information, making discharge summaries more consistently available during follow-up care.
Many physicians indicate a preference for quick voice mail updates on patients they’ve referred supported by the electronic or faxed record. This type of proactive communication is the basis of a strong and lasting referral relationship. In fact, the relationship can be further strengthened by tailoring communication to individual primary care doctors, according to their preferences.
Indeed, the most responsive specialists ask the referring physician how best to stay in touch because one size does not fit all. Some physicians prefer face-to-face contact, others phone or facsimile and still others e-mail. The use of electronic medical records and other electronic communication devices can help the physician enhance the consistency, speed and real time level of their physician-to-physician communication.
Primary care doctors want to work with specialists who recognize their role in treating the patient on an ongoing basis. Many want frequent communication about the plan of care and status. At the very least, tertiary specialists should always pay the courtesy of discharge communication—a phone call, e-mail, timely letter or fax when they return the patient to the community physician. The specialist should include the diagnosis, any issues that he or she may have identified; any changes in treatment and medication, follow-up recommendations and a phone or pager number if the referring physician has questions or concerns.
Both sides should keep each other informed of changes within their respective practice including new partnerships, expanded services, staff changes and insurance plan participation. Paying close attention to these relationship and communication basics builds trust and respect among colleagues and improves care to patients.
***

***
Systems Can Help With Communication
A cardiac surgeon in the Northeast with a very busy practice dictates immediately following each case, and then at the end of the day calls to update the referring physician even if he just leaves a voice mail with his pager number. The referring physician has 24/7 access to the cardiac surgeon, who, two weeks later, has his practice administrator send a thank-you note for the referral. At a conference of specialists who were questioning their own ability to commit to this level of time, he simply stated “how can you not afford to pay attention to this part of your practice?”
Another example involves a large specialty practice that was challenged with communication back to the referring physician. They hired a clinician to support them as patient/practice case manager, with a primary job focus on communicating about the patient, ensuring discharge information was forwarded and conducting a personal office call with the referring physician. This ensured it was received, understood and if not, helping the referring physician to gain quick access to the specialist.
Citations:
[i] “By the Numbers, 2008.” Society for Healthcare Strategy and Market Development of the American Hospital Association.
[ii] Sunil Kripalani, M.D., et al., “Deficits in Communication and Information Transfer Between Hospital-Based and Primary Care Physicians,” The Journal of the American Medical Association, Feb. 28 2007, 297; 831-841.
More:
- Our Healthcare Referral System is Broken
- Understanding the Referral Relationship in Medicine
- Physician Self-Referral “under arrangement” Scrutiny
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
- PRACTICES: www.BusinessofMedicalPractice.com
- HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
- CLINICS: http://www.crcpress.com/product/isbn/9781439879900
- ADVISORS: www.CertifiedMedicalPlanner.org
- FINANCE: Financial Planning for Physicians and Advisors
- INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors
- Dictionary of Health Economics and Finance
- Dictionary of Health Information Technology and Security
- Dictionary of Health Insurance and Managed Care


![]()
![]()
![]()

Share this:

Filed under: Health Insurance, Practice Management | Tagged: david marcinko, Doctor Referrals, Medical Provider Network Referral Leakage, patient referrals, SHSMD, Society for Healthcare Strategy and Market Development | 2 Comments »