











![]()
Forgetting ICD-9 … Moving on to ICD-10
[By Staff Reporters]
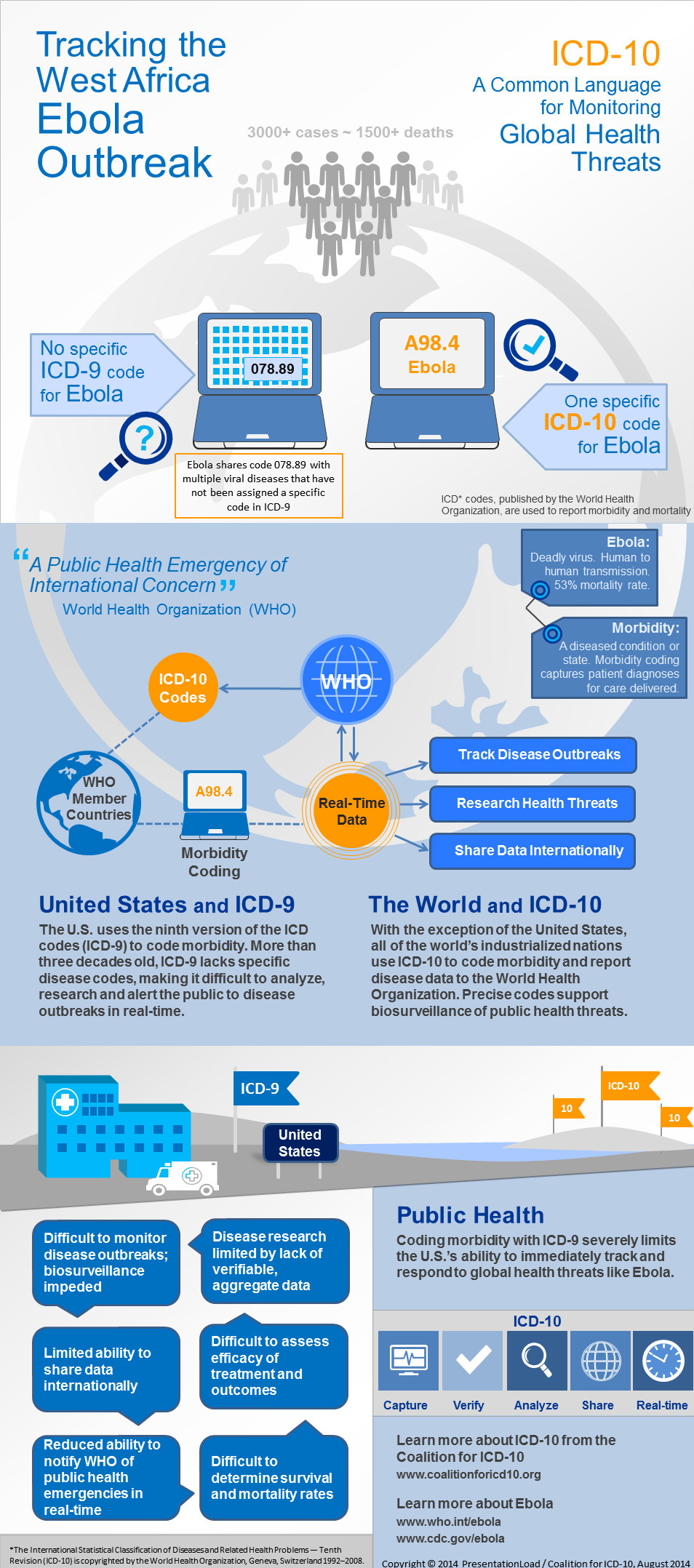
According to Tom Sullivan, there is no specific code for the Ebola virus under ICD-9?
And no, this is not a joke: There isn’t a specific one. Instead code number # 078.89 refers to multiple viral diseases. Under ICD-10, however, there is one. It’s A98.4.
***
***
The Proponent
That’s according to the Coalition for ICD-10 which, of course, is a proponent of moving to the new code set without further delay.
Assessment
The coalition’s main point is that specific codes can help public health officials better manage bio-surveillance. Do you agree?
Link: Infographic: ICD-10 could bolster Ebola biosurveillance
More: Ascel Bio on Forecasting Infectious Disease Outbreaks
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
- PHYSICIANS: www.MedicalBusinessAdvisors.com
- PRACTICES: www.BusinessofMedicalPractice.com
- HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
- CLINICS: http://www.crcpress.com/product/isbn/9781439879900
- ADVISORS: www.CertifiedMedicalPlanner.org
- BLOG: www.MedicalExecutivePost.com
- FINANCE: Financial Planning for Physicians and Advisors
- INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors

![]()
Share this:

Filed under: Ethics, Information Technology | Tagged: Ebola virus, ICD-10 |

Ebola and ICD-10?
I’m not sure that the 2014 Ebola outbreak is one of the greatest global health crises in recent history; but the past few days have brought forth a slew of alarming headlines:
• In Dallas, a nurse, Nina Pham, has become the first recorded case of Ebola transmission in the United States. Pham contracted the disease while treating a Liberian man, who died last week.
• A second nurse in Dallas has just been diagnosed.
• In Madrid, a nurse has contracted the disease after treating a missionary who had traveled to Sierra Leone.
• In response to the news from Dallas, the CDC intends to revise its Ebola guidelines for hospitals, though specifics have yet to be made public.
• Many experts are questioning the CDC’s existing recommendations, arguing that they’ve inadequately prepared hospitals to treat Ebola.
• In West Africa, over 4000 people are dead, with many children orphaned by the disease.
• The total mortality rate from the outbreak has risen to 70 percent.
So, an ICD-10 Ebola billing code seems meaningless in this regard.
Dr. David Edward Marcinko MBA
LikeLike
21 Days too Short?
A recent study on the quarantine period for Ebola virus suggests 21 days in isolation may not be enough. The incubation period for Ebola—time between the point of infection to the onset of symptoms—is two to 21 days, according to the World Health Organization.
http://currents.plos.org/outbreaks/article/on-the-quarantine-period-for-ebola-virus/
Yet, the CDC advises any individuals who were possibly exposed to the virus should monitor their health and restrict their travels for 21 days.
Dr. David Edward Marcinko MBA
LikeLike
Catastrophe Ebola: Protocols Versus Workflows
[The moron is the medium]
In Healthcare, the combination of a deficit in critical thinking and a surplus of arrogance leads to catastrophe. As of October 16, 2014, two nurses are being treated for Ebola infections.
On one hand, this is not a statistical catastrophe of millions of infected people. On the other, it is a catastrophe of breaches in critical-thinking on the part of government agencies such as the CDC and at least one proud hospital. Arrogance has for too long played a large role in Healthcare. Type I and Type II errors happen all the time. When they’re the result of arrogance, those errors are even more dangerous because they don’t receive the questioning they deserve.
Let’s look at why these two problems – sloppy thinking and arrogant attitude – led to the current situation.
There’s a difference between protocols and workflows. Where the CDC made its biggest error was to focus on protocols without considering the workflows within which those protocols operate.
It’s one thing to follow proper protection protocols in a low-variable, relatively static working environment. It’s quite another when the realities of nurse, physician, and other staff duties are factored in.
Have you ever worked in an isolation room? I have. If you haven’t, you might think all that’s involved is donning protective wear and letting high-tech infection control assets do their thing. Well, that’s a rather naive understanding of the reality.
The CDC and the Healthcare industry in general have missed this crucial point. Protocols, if they are to work effectively, must be developed with workflows in mind.
And by workflows, it’s not just the workflows within a facility. The workflows also involve the greater workflows of other facilities and agencies and societal infrastructures. In the case of the CDC, for instance, it does not appear that it develop all of the workflows required to do what it has the duty to do: Control. How can control possibly be achieved without workflows mapped-out with specific guidelines, processes, and human agency built-in?
As for critical thinking in wider contexts: much of the information concerning Ebola may be correct; however, viruses mutate – evolution is “smarter” than the brains it evolves. The simplicity of viral mechanisms is proof of the power of replication and tiny changes to ramify ecologies with novel systems.
All the (factual) knowledge tweeted and posted on social media, such as a 21-day incubation period or that it isn’t airborne may be true but there has been a layer of arrogance in belief without re-confirmation of the knowledge. I would not suggest paranoia – however, the arrogance would be “it’s definitely not possible to get Ebola via the airway”. The virus might not be transmissible as “airborne” but that does not mean Healthcare workers in close proximity of fluids can’t be infected from inhaled droplets. *Because* viruses mutate, it’s only responsible to continually vet our current assumptions through sieves of experimentation and research.
For example, what makes 21 such a magic number? It’s not a rhetorical question. It may indeed be “right”, but nature doesn’t follow *our* mathematics. We make observations and derive mathematical patterns from *them*. When dealing with mutable substances, it’s only rational to question empirical conclusions made during conditions which may no longer be exactly the same as they once were in healthcare settings.
The course of Ebola’s river of grief remains to be seen in the following months. Hopefully the situation has been contained or will be soon. Regardless, we need – more than ever – to critically and steadfastly re-think everything about what we think we know. The question mark is evolution’s crowning achievement.
In our time, media propagate messages faster than thought – the moron is the medium now, so we have to question diligently what we see. Even if the right information spreads, it’s ultimately the contextual application of that information that matters. That is to say: the accurate information can be inaccurately applied.
Yes, we need stringent protocols and we need to ensure that fully thought-through, mercilessly tested, and properly marketed protocols are followed. We also need to think about workflows. The two go together. And we can’t get them to operate smoothly, effectively, and safely when we have scarcities of thought and abundances of arrogance.
More thinking and questioning, less arrogance.
This is how our species has survived so far.
Phil Baumann RN
LikeLike
Ebola
Ban – Isolate and Quarantine; now!
Epidemiologist
LikeLike